

CD8-positive indolent T-Cell lymphoproliferative disorder of the gastrointestinal tract: A case report and review of literature
- PMID: 35801019
- PMCID: PMC9198890
- DOI: 10.12998/wjcc.v10.i15.4971
CD8-positive indolent T-Cell lymphoproliferative disorder of the gastrointestinal tract: A case report and review of literature
Abstract
Background: Indolent T-cell lymphoproliferative disorder of the gastrointestinal tract (ITLPD-GI), a primary tumor forming in the gastrointestinal (GI) tract, represents a rarely diagnosed clonal T-cell disease with a protracted clinical course.
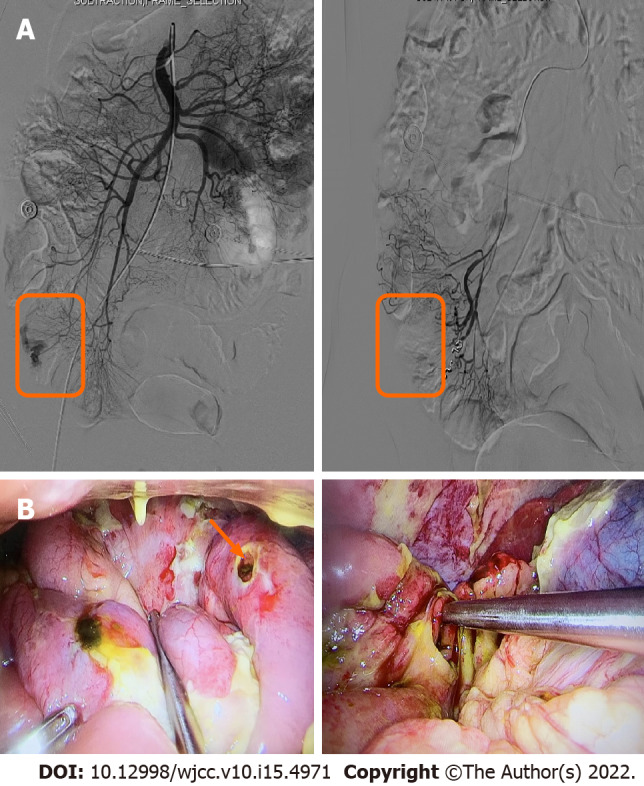
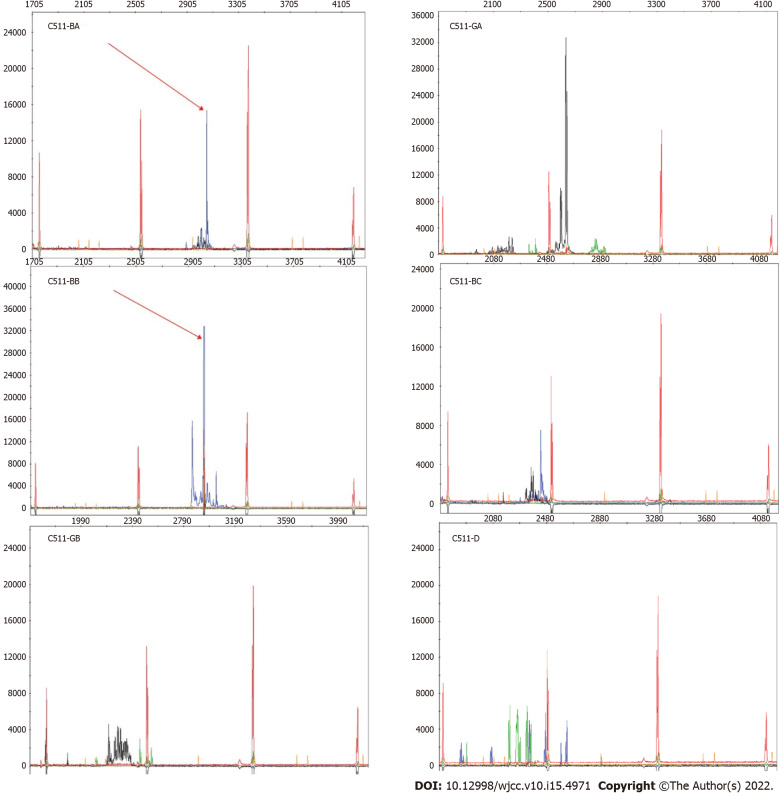
Case summary: This report presented a 45-year-old male patient with a 6-year history of anal fistula and a more than 10-year history of recurrent diarrhea who was not correctly diagnosed until the occurrence of complications such as intestinal perforation. Postsurgical histopathological analysis, combined with hematoxylin-eosin staining, immunohistochemistry and TCRβ/γ clonal gene rearrangement test, confirmed the diagnosis of CD8+ ITLPD-GI.
Conclusion: Individuals with this scarce lymphoma frequently show non-specific symptoms that are hard to recognize. So far, indolent CD8+ ITLPD-GI has not been comprehensively examined. The current mini-review focused on evaluating indolent CD8+ ITLPD-GI cases based on existing literature and discussing future directions for improved differential diagnosis, detection of genetic and epigenetic alterations, and therapeutic target identification.
Keywords: Case report; Gastrointestinal tract; Immunohistochemistry; Indolent T-cell lymphoproliferative disease; Inflammatory bowel disease.
©The Author(s) 2022. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: The authors declare that they have no competing interests.
Figures



References
-
- Chan JKC, Fukuyama M. Haematolymphoid tumours of the digestive system. In: WHO Classification of Tumours of the Digestive System, 5th ed. IARC: Lyon, France. 2019: 373–432.
-
- Jaffe ES, Chott A, Ott G, Chan JKC, Bhagat G, Tan SY, Stein H, Isaacson PG. Intestinal T-cell lymphoma. In WHO Classification of Tumours Haematopoietic and Lymphoid Tissues, Revised, 4th ed. IARC: Lyon, France. 2017: 372–380.
-
- Polyatskin IL, Artemyeva AS, Krivolapov YA. Revised WHO classification of tumors of hematopoietic and lymphoid tissues, 2017 (4th edition):lymphoid tumors. Arkh Patol. 2019;81:59–65. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
