

Hydropic leiomyoma: A radiologic pathologic correlation of a rare uterine tumor
- PMID: 35801124
- PMCID: PMC9253554
- DOI: 10.1016/j.radcr.2022.06.008
Hydropic leiomyoma: A radiologic pathologic correlation of a rare uterine tumor
Abstract
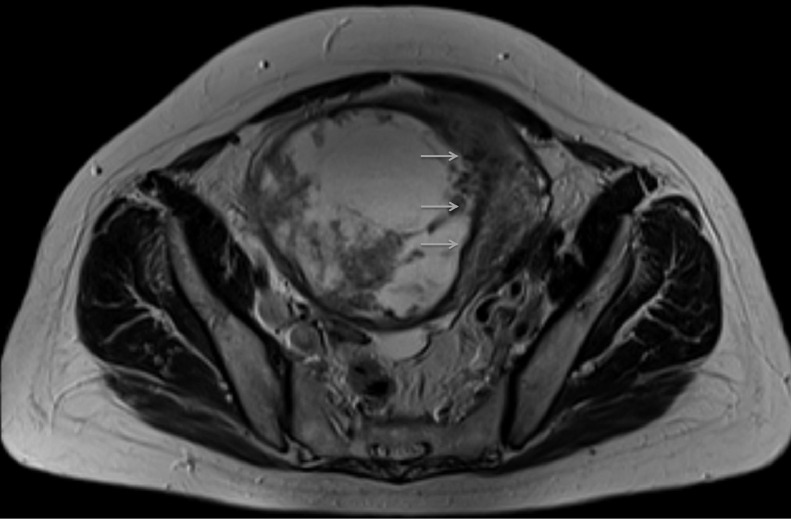
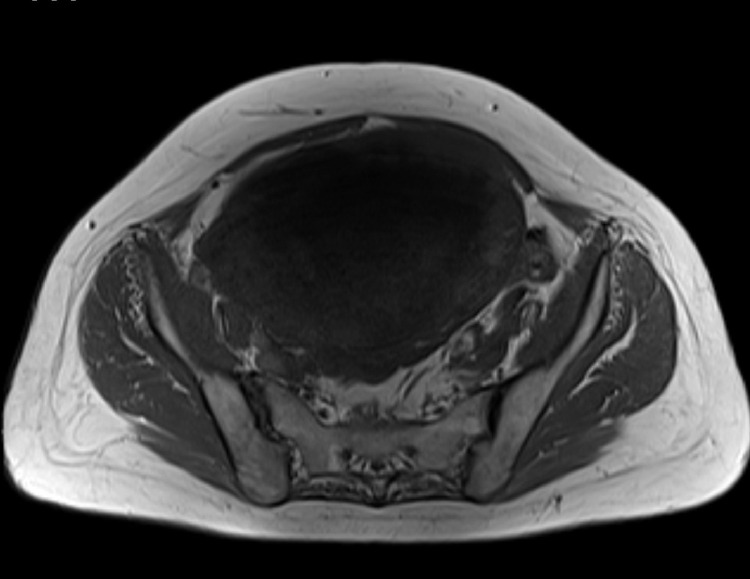
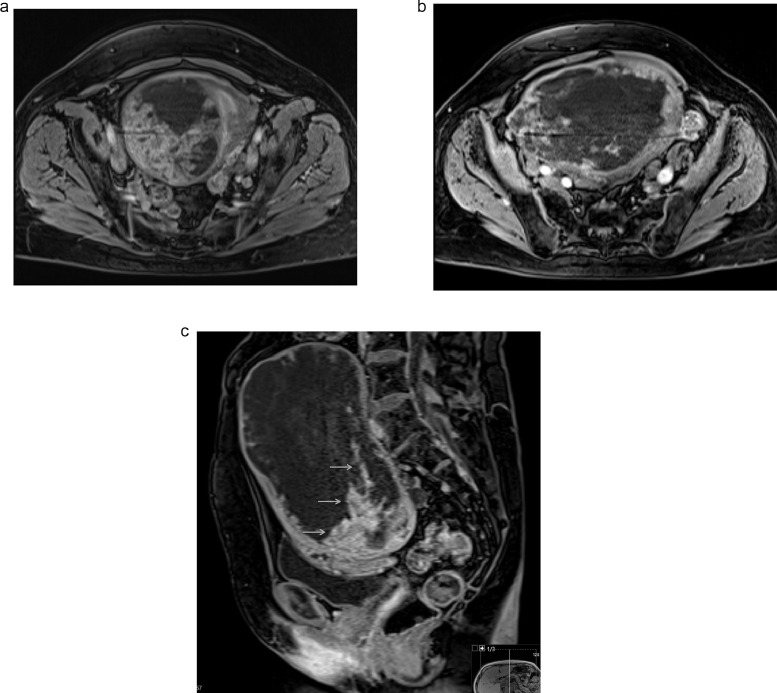
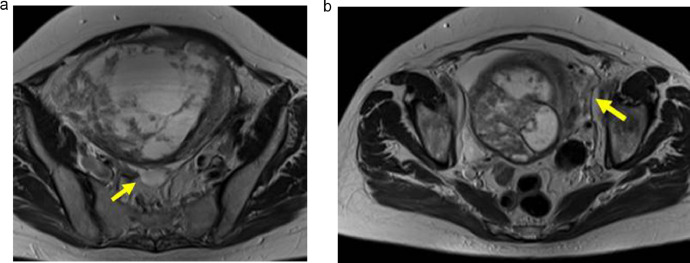
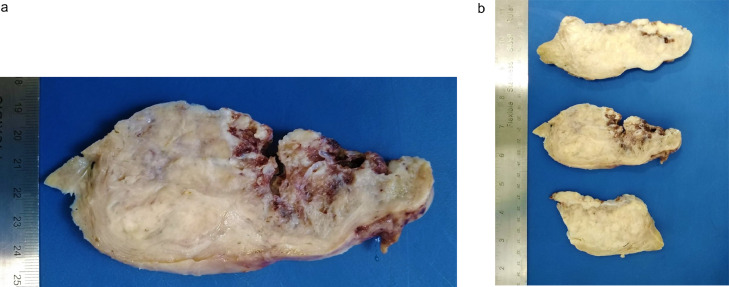
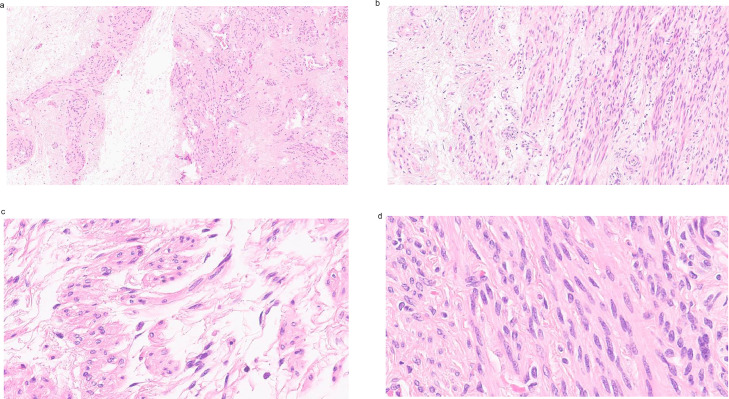
Hydropic leiomyoma is a rare leiomyoma subtype composed of a conspicuous zonal watery edematous stroma that causes compartmentalization of the smooth muscle cells. It exhibits atypical imaging features which can mimic malignancy, so differential diagnosis with malignant uterine tumors such as leiomyosarcoma is crucial for treatment decisions and patient follow-up. We describe the case of a 54-year-old postmenopausal woman presenting with a fast-growing abdominopelvic tumor associated with abdominal bloating, urinary frequency, and metrorrhagia. Radiologic evaluation depicted a voluminous, well-circumscribed, slightly lobulated, heterogeneous mass with mixed solid and cystic components arising from the uterus. Given the postmenopausal patient status, size of the tumor, and uncertainty about a possible malignant origin, an uneventful total abdominal hysterectomy with bilateral adnexectomy was performed as definitive treatment. However, as it is common practice in our institution, a second opinion report of the previous MRI was done before surgery, with the proposed diagnosis being hydropic leiomyoma. Pathologic examination of the surgical specimen revealed a large subserosal tumor with nodules separated by empty spaces and cysts due to watery exudate. Histologically, it was a mesenchymal neoplasm with trabecular and nested architecture, with tumor cells separated by watery fluid without mitosis or necrosis, securing the diagnosis of a hydropic leiomyoma.
Keywords: Atypical leiomyoma; Hydropic leiomyoma; Leiomyoma; Leiomyosarcoma; Uterus.
© 2022 The Authors. Published by Elsevier Inc. on behalf of University of Washington.
Figures

Similar articles
-
A subserosal, pedunculated, multilocular uterine leiomyoma with ovarian tumor-like morphology and histological architecture of adenomatoid tumors: a case report and review of the literature.J Med Case Rep. 2016 Dec 20;10(1):352. doi: 10.1186/s13256-016-1167-1. J Med Case Rep. 2016. PMID: 27998309 Free PMC article. Review.
-
Multinodular hydropic leiomyoma of the uterus with perinodular hydropic degeneration and extrauterine extension.Pathol Int. 2002 Aug;52(8):540-3. doi: 10.1046/j.1440-1827.2002.01380.x. Pathol Int. 2002. PMID: 12366814
-
Massive multilocular cystic leiomyoma of the uterus: an extreme example of hydropic degeneration.South Med J. 2007 Mar;100(3):309-12. doi: 10.1097/01.smj.0000257639.52322.7d. South Med J. 2007. PMID: 17396738
-
Hydropic leiomyoma of the uterus presenting as a giant abdominal mass.BMJ Case Rep. 2015 Sep 8;2015:bcr2015211929. doi: 10.1136/bcr-2015-211929. BMJ Case Rep. 2015. PMID: 26351316 Free PMC article.
-
Cotyledonoid leiomyoma: a benign uterine tumor with alarming gross appearance.Arch Pathol Lab Med. 2002 Feb;126(2):210-3. doi: 10.5858/2002-126-0210-CL. Arch Pathol Lab Med. 2002. PMID: 11825122 Review.
Cited by
-
AMH and Kisspeptin Receptor Expression in Rare Hydropic Leiomyoma: A Case Study.Am J Case Rep. 2025 Apr 30;26:e947953. doi: 10.12659/AJCR.947953. Am J Case Rep. 2025. PMID: 40305440 Free PMC article.
References
-
- WHO Classification of Tumours Editorial Board . Female genital tumours. 5th ed. IARC Press; Lyon: 2020. World Health Organization classification of tumours.
Publication types
LinkOut - more resources
Full Text Sources
