

Do paediatric early warning systems reduce mortality and critical deterioration events among children? A systematic review and meta-analysis
- PMID: 35801231
- PMCID: PMC9253845
- DOI: 10.1016/j.resplu.2022.100262
Do paediatric early warning systems reduce mortality and critical deterioration events among children? A systematic review and meta-analysis
Abstract
Aim: We conducted a systematic review and meta-analysis to answer the question: Does the implementation of Paediatric Early Warning Systems (PEWS) in the hospital setting reduce mortality, cardiopulmonary arrests, unplanned codes and critical deterioration events among children, as compared to usual care without PEWS?
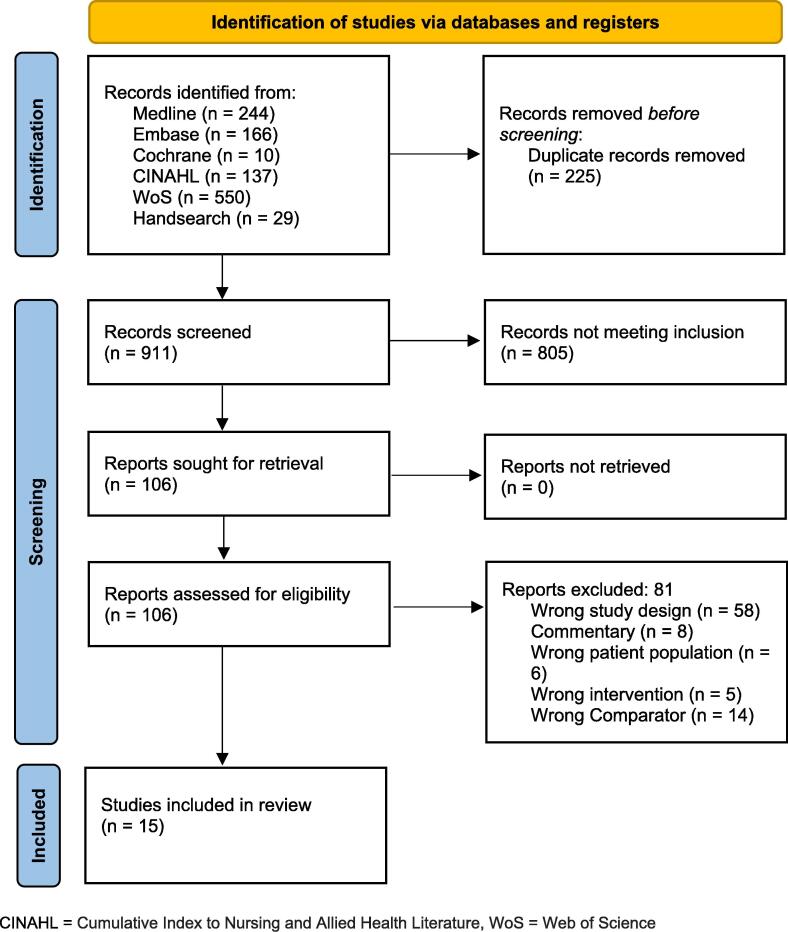
Methods: We conducted a comprehensive search using Medline, EMBASE, Cochrane Central Register of Controlled Trials, Cumulative Index to Nursing and Allied Health Literature and Web of Science. We included studies published between January 2006 and April 2022 on children <18 years old performed in inpatient units and emergency departments, and compared patient populations with PEWS to those without PEWS. We excluded studies without a comparator, case control studies, systematic reviews, and studies published in non-English languages. We employed a random effects meta-analysis and synthesised the risk and rate ratios from individual studies. We used the Scottish Intercollegiate Guidelines Network (SIGN) to appraise the risk of bias.
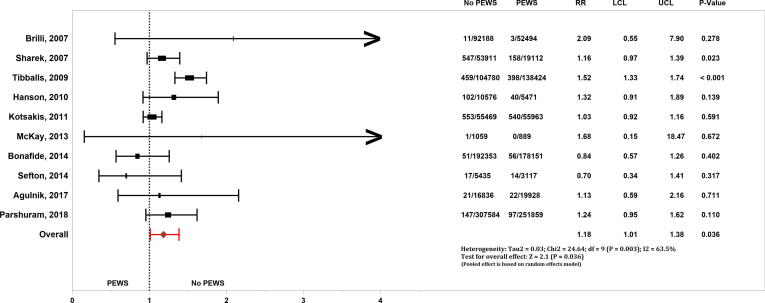
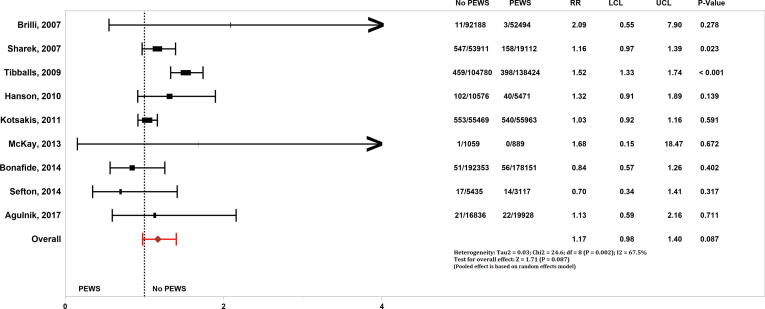
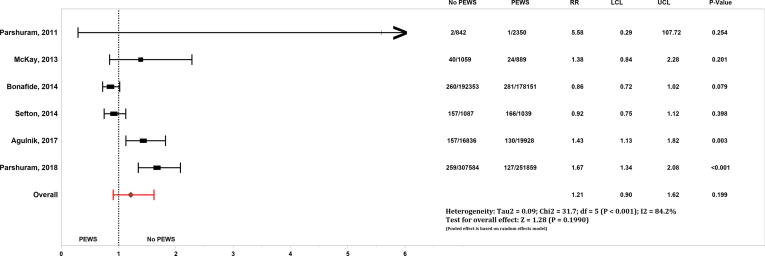
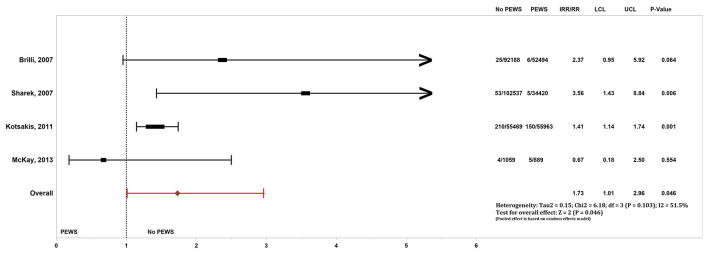
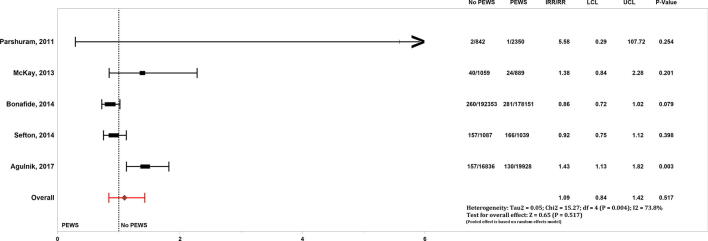
Results: Among 911 articles screened, 15 were included for descriptive analysis. Fourteen of the 15 studies were pre- versus post-implementation studies and one was a multi-centre cluster randomised controlled trial (RCT). Among 10 studies (580,604 hospital admissions) analysed for mortality, we found an increased risk (pooled RR 1.18, 95% CI 1.01-1.38, p = 0.036) in the group without PEWS compared to the group with PEWS. The sensitivity analysis performed without the RCT (436,065 hospital admissions) showed a non-significant relationship (pooled RR 1.17, 95% CI 0.98-1.40, p = 0.087). Among four studies (168,544 hospital admissions) analysed for unplanned code events, there was an increased risk in the group without PEWS (pooled RR 1.73, 95%CI 1.01-2.96, p = 0.046) There were no differences in the rate of cardiopulmonary arrests or critical deterioration events between groups. Our findings were limited by potential confounders and imprecision among included studies.
Conclusions: Healthcare systems that implemented PEWS were associated with reduced mortality and code rates. We recognise that these gains vary depending on resource availability and efferent response systems.PROSPERO registration: CRD42021269579.
Keywords: Child; Early Warning Scores; Mortality; Resuscitation.
© 2022 The Authors.
Figures
References
-
- Roland D. Paediatric early warning scores: Holy Grail and Achilles’ heel. Arch Dis Child Educ Pract Ed. 2012;97:208–215. - PubMed
-
- Sandell J.M., Maconochie I.K. Paediatric early warning systems (PEWS) in the ED. Emerg Med J. 2016;33:754–755. - PubMed
-
- Akre M., Finkelstein M., Erickson M., Liu M., Vanderbilt L., Billman G. Sensitivity of the pediatric early warning score to identify patient deterioration. Pediatrics. 2010;125:e763–e769. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
