

Intravenous fluid therapy in sepsis
- PMID: 35801708
- PMCID: PMC9463107
- DOI: 10.1002/ncp.10892
Intravenous fluid therapy in sepsis
Abstract
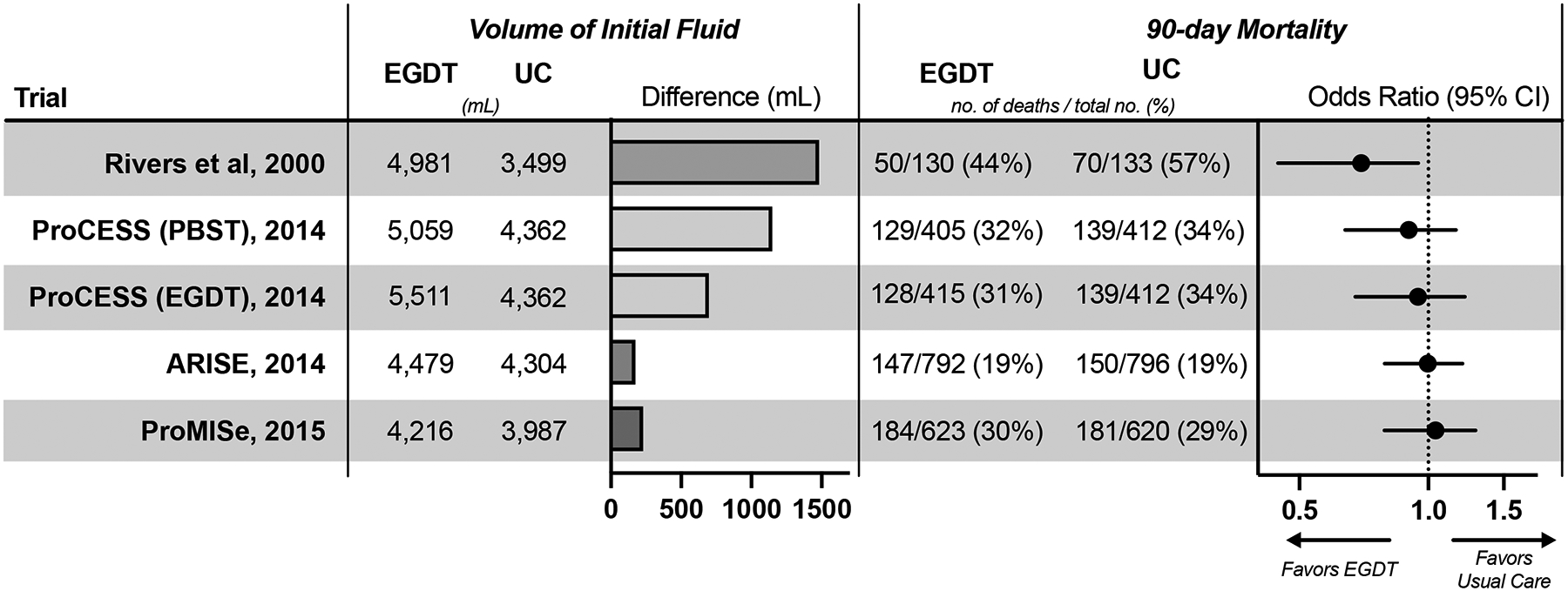
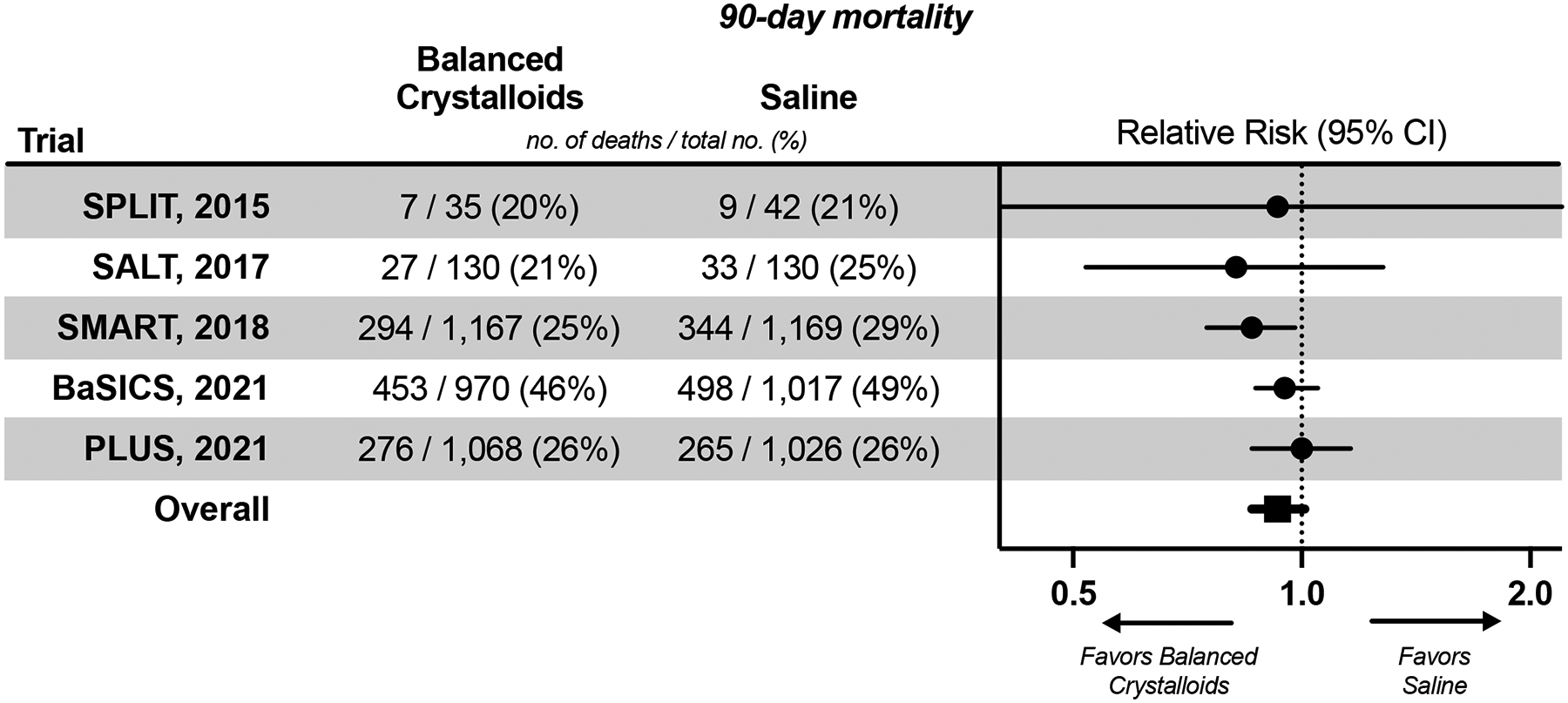
Sepsis is the dysregulated immune response to severe infection that is common and lethal among critically ill patients. Fluid administration is a common treatment for hypotension and shock in early sepsis. Fluid therapy can also cause edema and organ dysfunction. Research on the best treatment strategies for sepsis has provided insights on the optimal timing, dose, and type of fluid to treat patients with sepsis. Initial research on early goal-directed therapy for sepsis included an initial bolus of 30 ml/kg of fluid, but more recent research has supported use of smaller volumes. After initial fluid resuscitation, minimizing additional fluid administration may be beneficial, but no single measure has been established as the best method to guide ongoing fluid management in sepsis. Dynamic measures of "fluid responsiveness" can predict which patients will experience an increase in cardiac output from a fluid bolus. Use of such a measure in clinical care remains limited by applicability to patient populations and uncertainty regarding the effect on clinical outcomes. Recent research informs the effect of fluid composition on outcomes for patients with sepsis. Current data support the use of balanced crystalloids, rather than saline, and the use of crystalloids, rather than semisynthetic colloids. The role for albumin administration in sepsis remains uncertain. Future research should focus on determining the optimal volume of fluid during sepsis resuscitation, the effectiveness of measures of "fluid responsiveness" in improving outcomes, the optimal composition of crystalloid solutions, the role of albumin, and the effects of "deresuscitation" after septic shock.
Keywords: albumin; colloids; critical illness; crystalloid solutions; fluid resuscitation; intravenous fluid; sepsis.
© 2022 American Society for Parenteral and Enteral Nutrition.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
