

Semi-occlusive management of fingertip injuries with finger caps: A randomized controlled trial in children and adults
- PMID: 35801770
- PMCID: PMC9259139
- DOI: 10.1097/MD.0000000000029324
Semi-occlusive management of fingertip injuries with finger caps: A randomized controlled trial in children and adults
Abstract
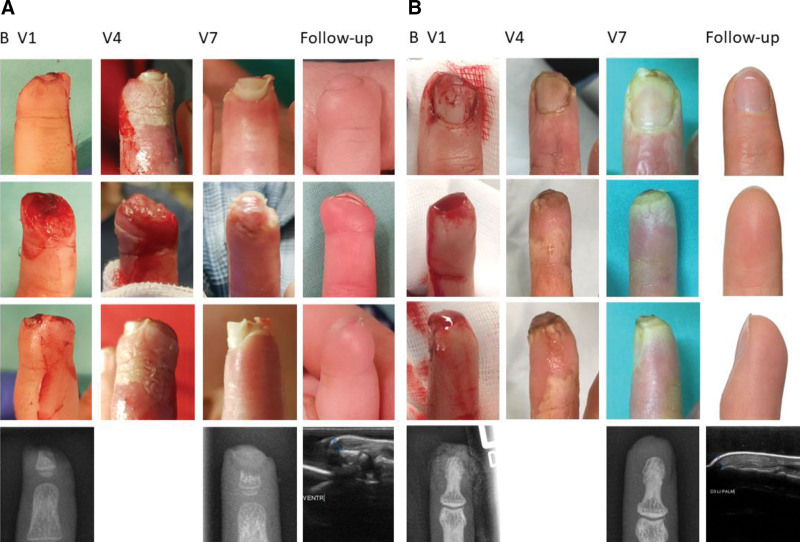
Background: Human fingertips can regenerate functionally and cosmetically excellent skin and soft tissues. Physiological conditions suppress scar formation and are thus a prerequisite for regenerative healing. Self-adhesive film dressings can provide such favorable conditions. The semi-occlusive treatment is superior to surgery. However, standard dressings leak malodorous wound fluid eventually until the wound is dry. Therefore, we developed and tested a silicone finger cap that forms a mechanically protected, wet chamber around the injury. Its puncturable reservoir allows access to the wound fluid for diagnostic and research purposes and the delivery of pro-regenerative drugs in the future.
Methods: Patients >2 years with full-thickness fingertip injuries unsuitable for simple primary closure were randomized to start treatment with either the film dressing or the silicone finger cap. After 2 weeks, we changed to the other treatment. Patients' choice on the preferred treatment after 4 weeks was the primary outcome parameter. Additionally, we monitored adverse events, unplanned visits, tissue gain, functionality, cosmetic outcome, and quality of life.
Results: We randomized 11 patients 2 to 72 years to each group. Eighteen to 20 (90%, intention-to-treat) patients preferred the finger cap. All patients were satisfied with the cosmetic outcome, 88.9% had no disturbing sensibility changes, and 73.7% could report no distortion in the finger's daily use. Epithelialization took between 5 weeks for Allen II and up to 9 weeks in Allen IV injuries. There were 19 device-related adverse events under film dressing and 13 under the finger cap. There were neither severe adverse device effects nor unexpected severe adverse device effects.
Conclusion: Employing the summative or synthetic primary endpoint "patient decision for one or the other procedure," our pseudocross-over-designed RCT succeeded in statistically significantly demonstrating the superiority of the silicone finger cap over conventional film therapy. The finger cap was safe and effective, reaching excellent results on all treated injuries without any need for disinfection, antibiotics, shortening of protruding bones, or treatment of hypergranulations. Distal to the tendon insertions, we did not see any limitations regarding injury mechanism, amputation plane, or patients' age.
Copyright © 2022 the Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The TU-Dresden, Dr Jurek Schultz, and Prof Guido Fitze have filed a patent for the silicone finger cap (PCT/DE2014/100088; 14721743.4-1308; 14/774,997). Besides, the authors declared no potential conflicts of interest with respect to the research, authorship, and publication of this study protocol. Randomization, monitoring, evaluation of study data, statistics and sponsor office are committed to the KKS Dresden, an institute independent of the Department of Pediatric Surgery.
Figures

References
-
- Conn JM, Annest JL, Ryan GW, et al. Non-work-related finger amputations in the United States, 2001-2002. Ann Emerg Med. 2005;45:630–5. - PubMed
-
- Macgregor DM, Hiscox JA. Fingertip trauma in children from doors. Scott Med J. 1999;44:114–5. - PubMed
-
- Ljungberg E, Rosberg HE, Dahlin LB. Hand injuries in young children. J Hand Surg Am. 2003;28 B(4):376–380. - PubMed
-
- Muneuchi G, Tamai M, Igawa K, et al. The PNB classification for treatment of fingertip injuries: the boundary between conservative treatment and surgical treatment. Ann Plast Surg. 2005;54:604–9. - PubMed
-
- Illingworth CM. Trapped fingers and amputated finger tips in children. J Pediatr Surg. 1974;9:853–58. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
