

Comparison of Six-Minute Walk Test and Modified Bruce Treadmill Test in Paediatric Patients With Severe Burns: A Cross-Over Study
- PMID: 35801864
- PMCID: PMC9593470
- DOI: 10.2340/jrm.v54.1064
Comparison of Six-Minute Walk Test and Modified Bruce Treadmill Test in Paediatric Patients With Severe Burns: A Cross-Over Study
Abstract
Objective: To compare the six-minute walk test and the Modified Bruce treadmill test in paediatric patients with severe burns.
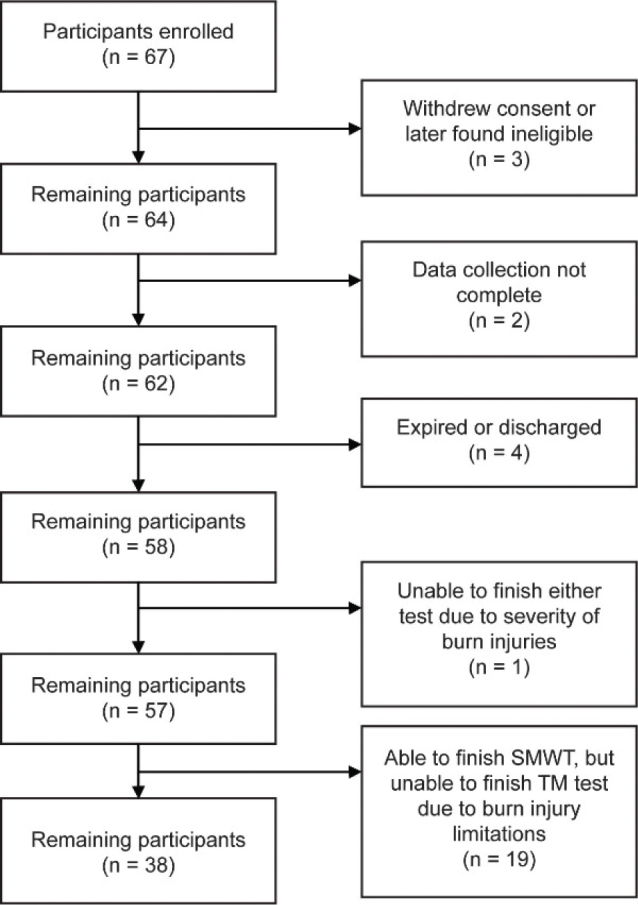
Subjects: A total of 67 children, aged 7-17 years, with severe burns.
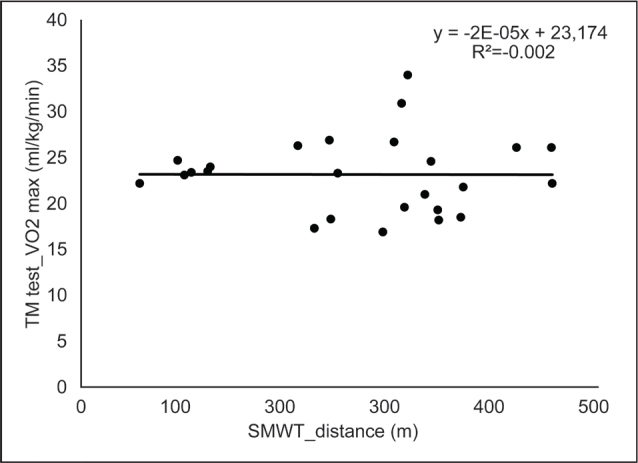
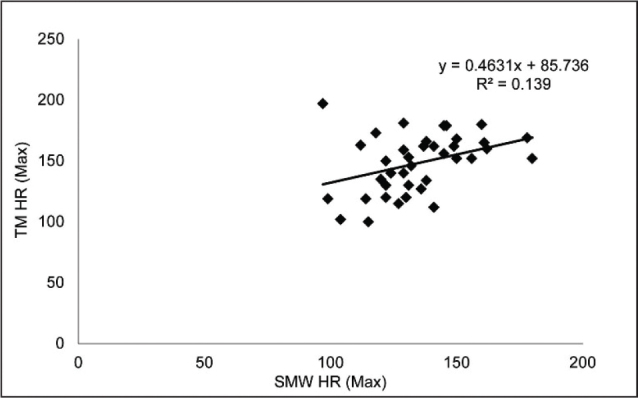
Methods: Participants were assigned to perform the six-minute walk test and the Modified Bruce treadmill test in randomized order on discharge from acute burn care. Primary outcome measure was heart rate. Secondary outcome measures were distance walked, Borg's CR-10 rate of perceived exertion, and maximal oxygen uptake (VO2).
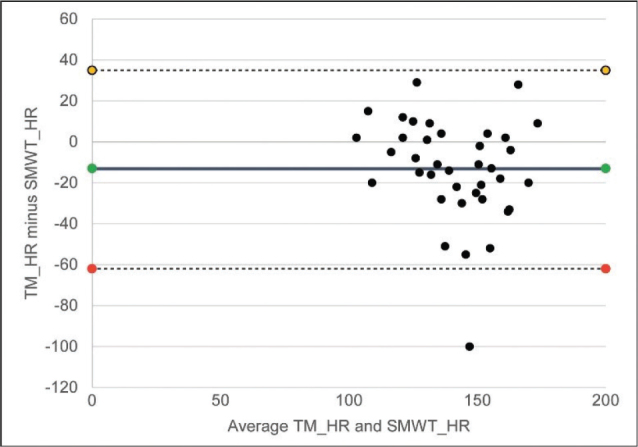
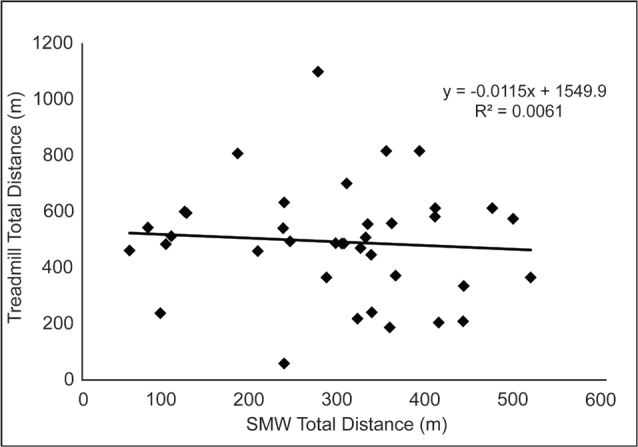
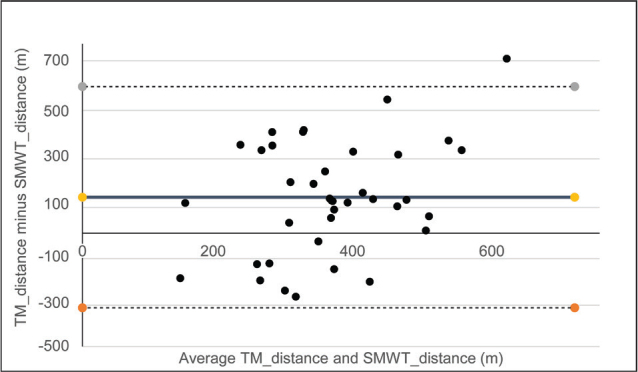
Results: A total of 67 participants were enrolled. Thirty-eight patients completed both tests. The mean six-minute walk test maximum heart rate was 135 ± 19 bpm (range 97-180 bpm) and the mean Modified Bruce treadmill test maximum heart rate was 148 ± 24 bpm (range 100-197 bpm; p ≤ 0.05), with a weak positive correlation of R² = 0.14. The mean six-minute walk test maximum distance was 294 ± 124 m (range 55 to 522 m) while the mean Modified Bruce treadmill test maximum distance was 439 ± 181 m (range 53 to 976 m; p ≤ 0.05), with no correlation of R² = 0.006. The mean RPE CR-10 score for the six-minute walk test was 3 ± 2.5 (range 0-10) vs a mean RPE CR-10 score of 10 ± 0 for the Modified Bruce treadmill test.
Conclusion: The Modified Bruce treadmill test challenges the cardiorespiratory system significantly more than the six-minute walk test, as reflected by maximum heart rate measurements, and the perception of effort (i.e. rate of perceived exertion) by the patient. When possible, the Modified Bruce treadmill test should be used to assess cardiovascular functional capacity. However, the six-minute walk test may be more clinically feasible for use with paediatric patients with burns, and provides information about submaximal functional exercise capacity.
Conflict of interest statement
Figures
Similar articles
-
Comparing 6-minute walk versus treadmill walking distance as outcomes in randomized trials of peripheral artery disease.J Vasc Surg. 2020 Mar;71(3):988-1001. doi: 10.1016/j.jvs.2019.05.058. Epub 2019 Dec 23. J Vasc Surg. 2020. PMID: 31870756 Free PMC article.
-
Clinical correlates and prognostic significance of six-minute walk test in patients with primary pulmonary hypertension. Comparison with cardiopulmonary exercise testing.Am J Respir Crit Care Med. 2000 Feb;161(2 Pt 1):487-92. doi: 10.1164/ajrccm.161.2.9906015. Am J Respir Crit Care Med. 2000. PMID: 10673190
-
Comparative analysis of oxygen uptake in elderly subjects performing two walk tests: the six-minute walk test and the 200-m fast walk test.Clin Rehabil. 2008 Feb;22(2):162-8. doi: 10.1177/0269215507080125. Clin Rehabil. 2008. PMID: 18212036
-
[The 6 minute walking test: a cost-effective alternative to spiro-ergometry in patients with chronic heart failure?].Z Kardiol. 2000 Feb;89(2):72-80. doi: 10.1007/s003920050012. Z Kardiol. 2000. PMID: 10768274 Review. German.
-
Submaximal Field Walking Tests Applied in the Cardiopulmonary Assessment in Congenital Heart Diseases: A Systematic Review.Curr Pediatr Rev. 2024;21(1):56-66. doi: 10.2174/0115733963263592231127042702. Curr Pediatr Rev. 2024. PMID: 38251699
Cited by
-
[Prospective study on the effects of resistance training with elastic band at home on muscle function and walking ability of severely burned children].Zhonghua Shao Shang Yu Chuang Mian Xiu Fu Za Zhi. 2023 Dec 20;39(12):1131-1139. doi: 10.3760/cma.j.cn501225-20230729-00022. Zhonghua Shao Shang Yu Chuang Mian Xiu Fu Za Zhi. 2023. PMID: 38129299 Free PMC article. Clinical Trial. Chinese.
References
-
- American Burn Association . Burn Incidence Fact Sheet. Burn incidence and treatment in the United States: 2016 [serial on the internet]. 2020. [cited 2021 Dec 3]. Available from: https://ameriburn.org/who-we-are/media/burn-incidence-fact-sheet/
-
- Bloomfield SA. Changes in musculoskeletal structure and function with prolonged bed rest. Med Sci Sports Exerc 1997; 29: 197–206. - PubMed
-
- de Lateur BJ, Magyar-Russell G, Bresnick MG, Bernier FA, Ober MS, Krabak BJ, et al. . Augmented exercise in the treatment of deconditioning from major burn injury. Arch Phys Med Rehabil 2007; 88: S18–23. - PubMed
