

Effects of an amino acid buffered hypochlorite solution as an adjunctive to air-powder abrasion in open-flap surface decontamination of implants failed for peri-implantitis: an ex vivo randomized clinical trial
- PMID: 35802191
- PMCID: PMC9889426
- DOI: 10.1007/s00784-022-04608-5
Effects of an amino acid buffered hypochlorite solution as an adjunctive to air-powder abrasion in open-flap surface decontamination of implants failed for peri-implantitis: an ex vivo randomized clinical trial
Abstract
Objectives: To evaluate ex vivo the efficacy of an amino acid buffered hypochlorite solution supplemented to surface debridement with air-powder abrasion in removing bacterial biofilm following open-flap decontamination of implants failed due to peri-implantitis.
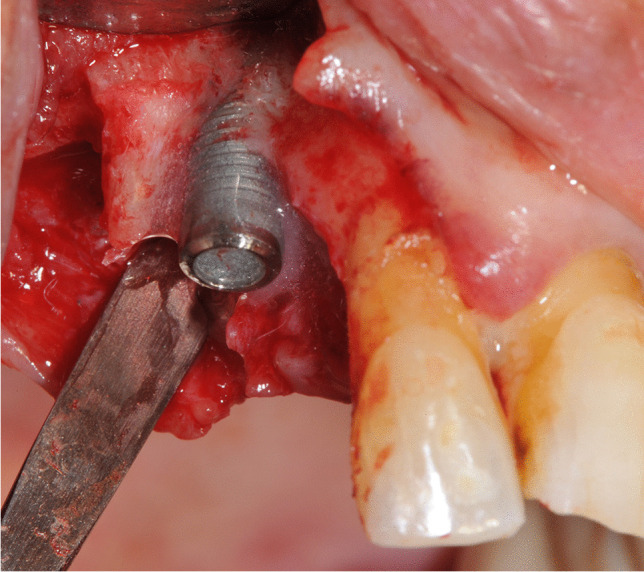
Materials and methods: This study was an ex vivo, single-blind, randomized, intra-subject investigation. Study population consisted of 20 subjects with at least three implants failed for peri-implantitis (in function for > 12 months and progressive bone loss exceeding 50%) to be explanted. For each patient, implants were randomly assigned to surface decontamination with sodium bicarbonate air-powder abrasion (test-group 1) or sodium bicarbonate air-powder abrasion supplemented by amino acid buffered hypochlorite solution (test-group 2) or untreated control group. Following open-flap surgery, untreated implants (control group) were explanted. Afterwards, test implants were decontaminated according to allocation and explanted. Microbiological analysis was expressed in colony-forming units (CFU/ml).
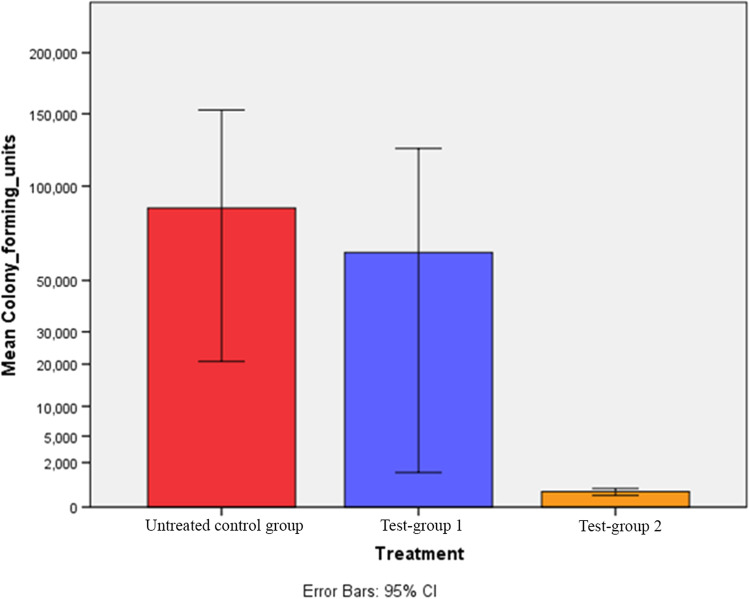
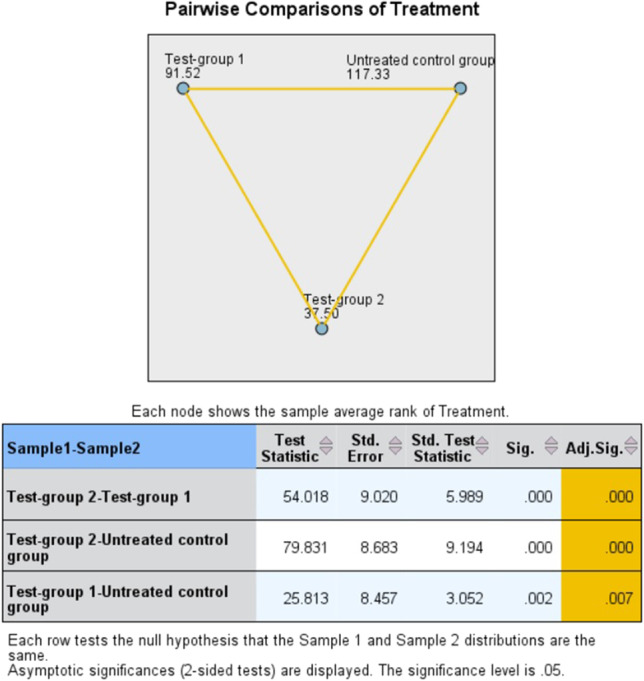
Results: A statistically significant difference in the concentrations of CFU/ml was found between implants of test-group 1 (63,018.18 ± 228,599.36) (p = 0.007) and implants of test-group 2 (260.00 ± 375.80) (p < 0.001) compared to untreated implants (control group) (86,846.15 ± 266,689.44). The concentration of CFU/ml on implant surfaces was lower in test-group 2 than in test-group 1, with a statistically significant difference (p < 0.001).
Conclusion: The additional application of amino acid buffered hypochlorite solution seemed to improve the effectiveness of implant surface decontamination with air-powder abrasion following open-flap surgery.
Clinical relevance: Lacking evidence on the most effective method for biofilm removal from contaminated implant surfaces, the present experimental study provides further information for clinicians and researchers.
Keywords: Air-powder abrasion; Biofilms; Chemical decontamination; Dental implant; Microbiota; Peri-implantitis.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
The authors declare no competing interests.
Figures
Similar articles
-
Comparison of the effects of air-powder abrasion, chemical decontamination, or their combination in open-flap surface decontamination of implants failed for peri-implantitis: an ex vivo study.Clin Oral Investig. 2021 May;25(5):2667-2676. doi: 10.1007/s00784-020-03578-w. Epub 2020 Sep 25. Clin Oral Investig. 2021. PMID: 32975703 Free PMC article. Clinical Trial.
-
Cold atmospheric plasma coupled with air abrasion in liquid medium for the treatment of peri-implantitis model grown with a complex human biofilm: an in vitro study.Clin Oral Investig. 2021 Dec;25(12):6633-6642. doi: 10.1007/s00784-021-03949-x. Epub 2021 Apr 24. Clin Oral Investig. 2021. PMID: 33893556 Free PMC article.
-
Air-Abrasive Disinfection of Implant Surfaces in a Simulated Model of Periimplantitis.Implant Dent. 2017 Jun;26(3):423-428. doi: 10.1097/ID.0000000000000597. Implant Dent. 2017. PMID: 28486355
-
Efficacy of Decontamination Methods for Biofilm Removal from Dental Implant Surfaces and Reosseointegration: An AAP/AO Systematic Review on Peri-implant Diseases and Conditions.Int J Oral Maxillofac Implants. 2025 Jun 6;(4):91-160. Int J Oral Maxillofac Implants. 2025. PMID: 40476898
-
[Peri-implantitis: tools and techniques for disinfecting the implant surface].Schweiz Monatsschr Zahnmed. 2011;121(4):341-55. Schweiz Monatsschr Zahnmed. 2011. PMID: 21574511 Review. French, German. No abstract available.
References
-
- Berglundh T, Armitage G, Araujo MG, et al. Peri-implant diseases and conditions: consensus report of workgroup 4 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J Periodontol. 2018;89(Suppl 1):313–318. doi: 10.1002/JPER.17-0739. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
