

Supporting Structured Data Capture for Patients With Cancer: An Initiative of the University of Wisconsin Carbone Cancer Center Survivorship Program to Improve Capture of Malignant Diagnosis and Cancer Staging Data
- PMID: 35802837
- PMCID: PMC9296185
- DOI: 10.1200/CCI.22.00020
Supporting Structured Data Capture for Patients With Cancer: An Initiative of the University of Wisconsin Carbone Cancer Center Survivorship Program to Improve Capture of Malignant Diagnosis and Cancer Staging Data
Abstract
Purpose: Structured data elements within electronic health records are health-related information that can be entered, stored, and extracted in an organized manner at later time points. Tracking outcomes for cancer survivors is also enabled by structured data. We sought to increase structured data capture within oncology practices at multiple sites sharing the same electronic health records.
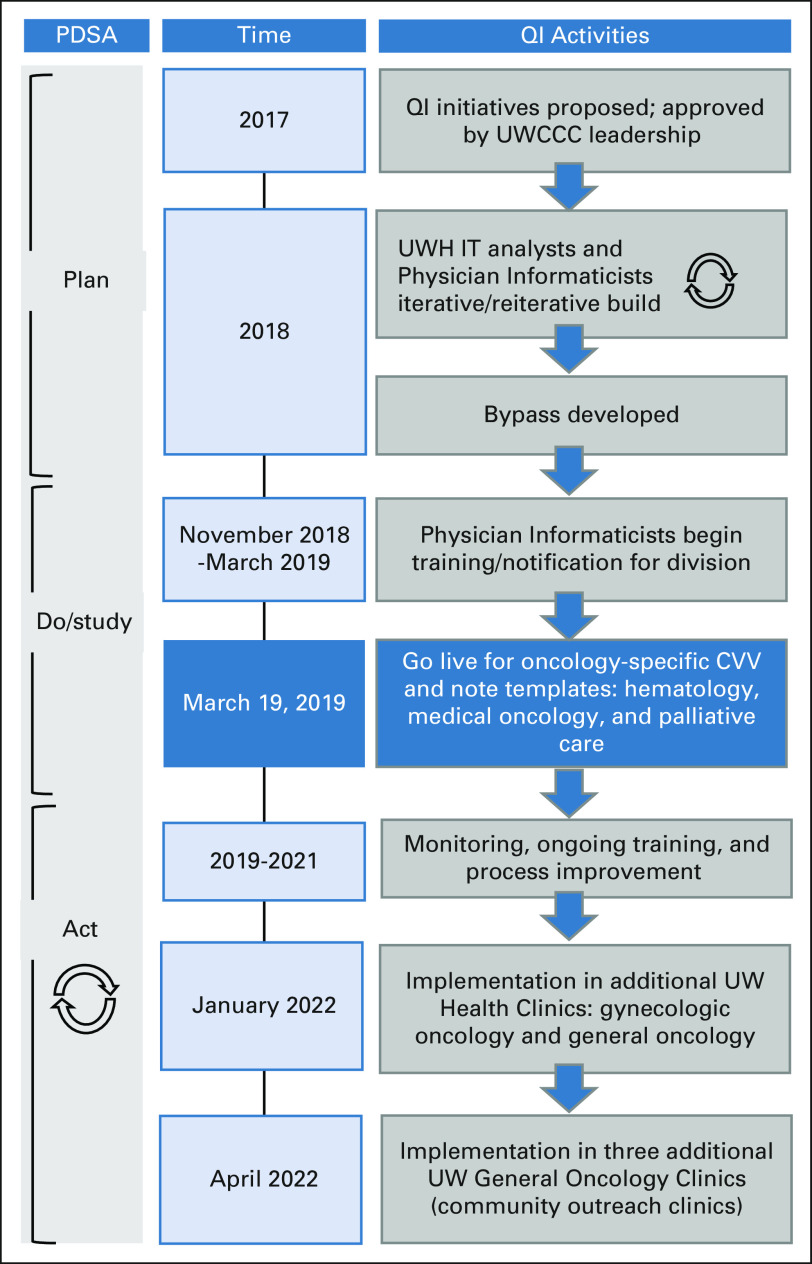
Methods: Applying engineering approaches and the Plan-Do-Study-Act cycle, we launched dual quality improvement initiatives to ensure that a malignant diagnosis and stage were captured as structured data. Intervention: Close Visit Validation (CVV) requires providers to satisfy certain criteria before closing ambulatory encounters. CVV may be used to track open clinical encounters and chart delinquencies to encourage optimal clinical workflows. We added two cancer-specific required criteria at the time of closing encounters in oncology clinics: (1) the presence of at least one malignant diagnosis on the Problem List and (2) staging all the malignant diagnoses on the Problem List when appropriate.
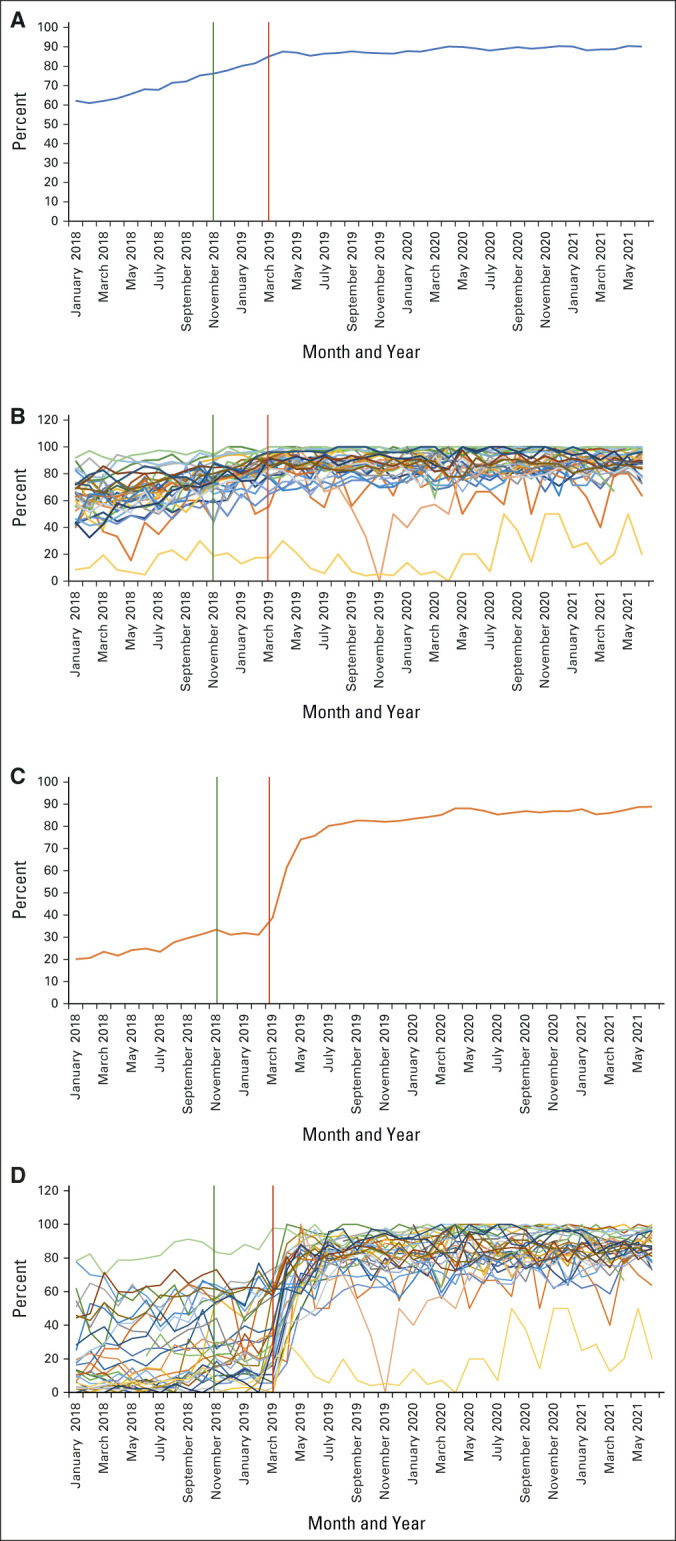
Results: Six months before the CVV implementation, the percentage of encounters with a malignant diagnosis on the Problem List at the time of the encounter was 65%, whereas the percentage of encounters with a staged diagnosis was 32%. Three months after cancer-specific CVV implementation, the percentages were 85% and 75%, respectively. Rates had increased to 90% and 88% more than 2 years after implementation.
Conclusion: Oncologist performance improved after the implementation of cancer-specific CVV criteria, with persistently high percentages of relevant malignant diagnoses and cancer stage structured data capture 2 years after the intervention.
Conflict of interest statement
No other potential conflicts of interest were reported.
Figures
References
-
- Häyrinen K, Saranto K.The core data elements of electronic health record in Finland Stud Health Technol Inform 116131–1362005 - PubMed
-
- Ehrenstein V, Kharrazi H, Lehmann H, et al. Obtaining data from electronic health records. In: Gliklich RE, Leavy MB, Dreyer NA, editors. Tools and Technologies for Registry Interoperability, Registries for Evaluating Patient Outcomes: A User's Guide. ed 3, Addendum 2. Rockville, MD: Agency for Healthcare Research and Quality (US); 2019. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
