

A classification and regression tree analysis identifies subgroups of childhood type 1 diabetes
- PMID: 35803018
- PMCID: PMC9270253
- DOI: 10.1016/j.ebiom.2022.104118
A classification and regression tree analysis identifies subgroups of childhood type 1 diabetes
Abstract
Background: Diabetes in childhood and adolescence includes autoimmune and non-autoimmune forms with heterogeneity in clinical and biochemical presentations. An unresolved question is whether there are subtypes, endotypes, or theratypes within these forms of diabetes.
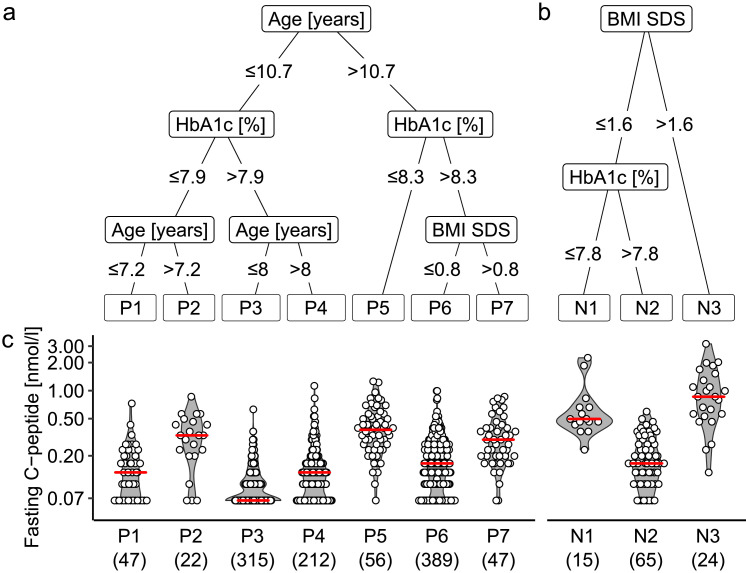
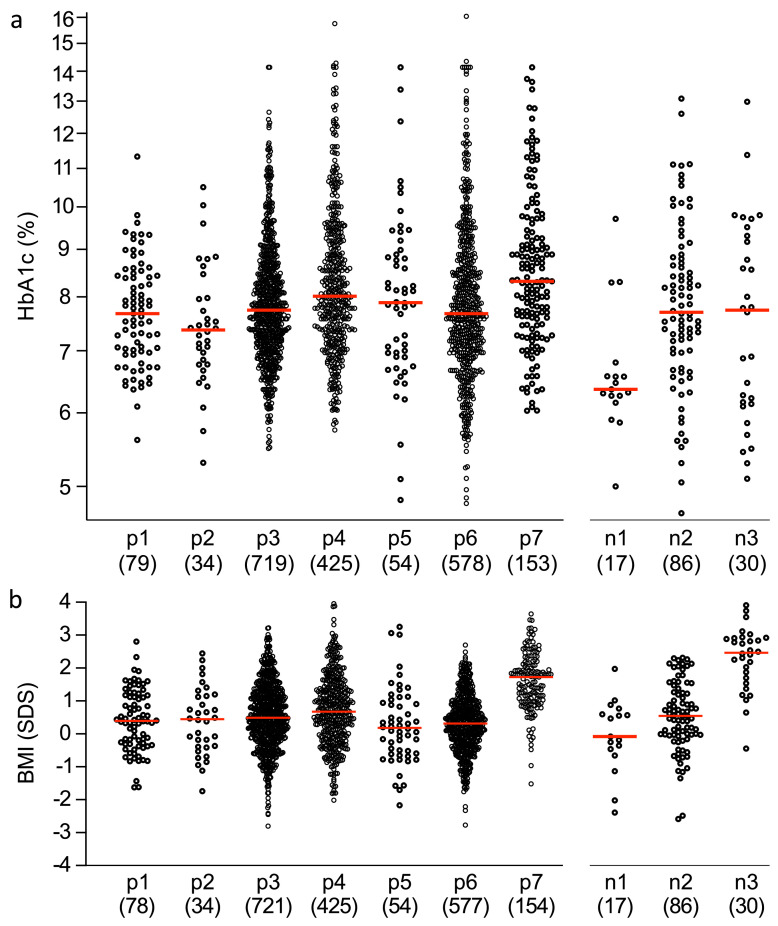
Methods: The multivariable classification and regression tree (CART) analysis method was used to identify subgroups of diabetes with differing residual C-peptide levels in patients with newly diagnosed diabetes before 20 years of age (n=1192). The robustness of the model was assessed in a confirmation and prognosis cohort (n=2722).
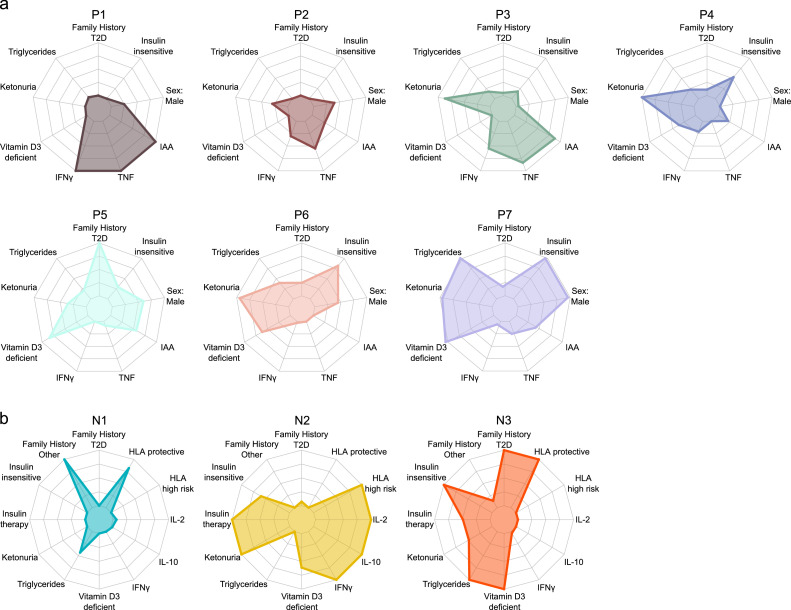
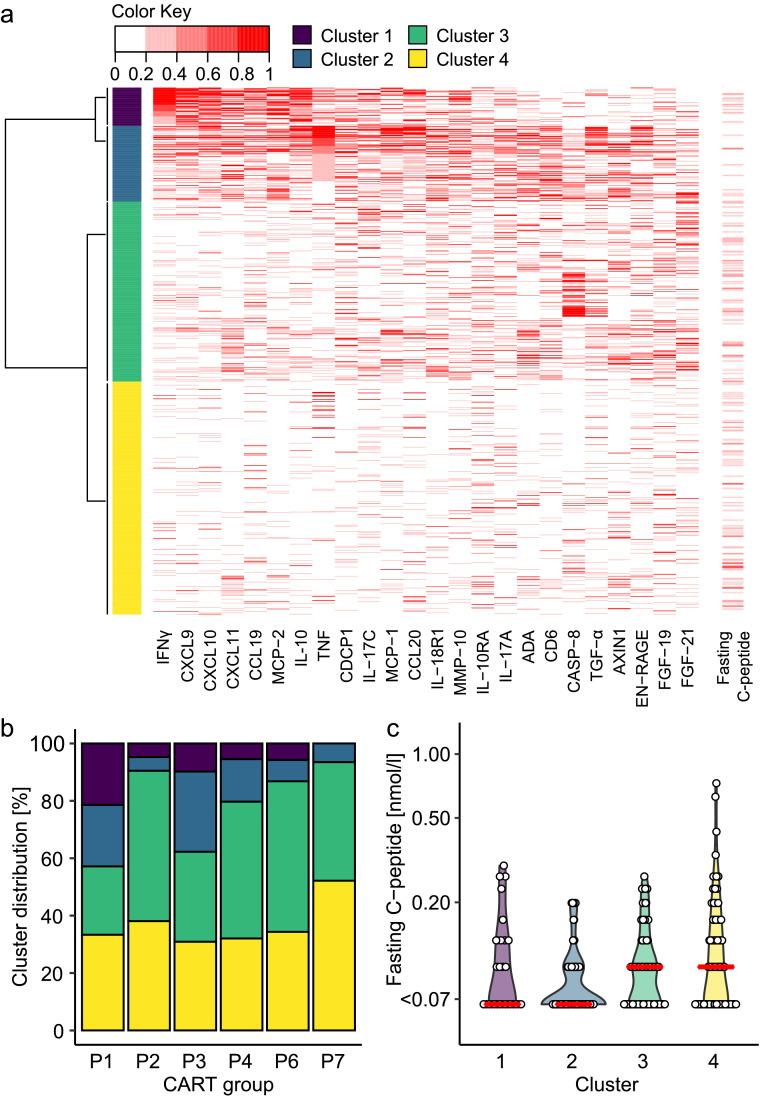
Findings: The analysis selected age, haemoglobin A1c (HbA1c), and body mass index (BMI) as split parameters that classified patients into seven islet autoantibody-positive and three autoantibody-negative groups. There were substantial differences in genetics, inflammatory markers, diabetes family history, lipids, 25-OH-Vitamin D3, insulin treatment, insulin sensitivity and insulin autoimmunity among the groups, and the method stratified patients with potentially different pathogeneses and prognoses. Interferon-ɣ and/or tumour necrosis factor inflammatory signatures were enriched in the youngest islet autoantibody-positive groups and in patients with the lowest C-peptide values, while higher BMI and type 2 diabetes characteristics were found in older patients. The prognostic relevance was demonstrated by persistent differences in HbA1c at 7 years median follow-up.
Interpretation: This multivariable analysis revealed subgroups of young patients with diabetes that have potential pathogenetic and therapeutic relevance.
Funding: The work was supported by funds from the German Federal Ministry of Education and Research (01KX1818; FKZ 01GI0805; DZD e.V.), the Innovative Medicine Initiative 2 Joint Undertaking INNODIA (grant agreement No. 115797), the German Robert Koch Institute, and the German Diabetes Association.
Keywords: C-peptide; CART analysis; Childhood autoimmune disease; Diabetes endotypes; Diabetes in childhood; Inflammation; Islet autoantibody; Obesity; Type 1 diabetes genetic susceptibility.
Copyright © 2022 The Author(s). Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of interests The authors have declared that no competing interests exist.
Figures
References
-
- Patterson CC, Karuranga S, Salpea P, et al. Worldwide estimates of incidence, prevalence and mortality of type 1 diabetes in children and adolescents: results from the International Diabetes Federation Diabetes Atlas, 9th edition. Diabetes Res Clin Pract. 2019;157 - PubMed
-
- American Diabetes Association. 2 Classification and diagnosis of diabetes: standards of medical care in diabetes—2020. Diabetes Care. 2020;43(suppl 1):S14–S31. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
