

Multivariable Prediction Model for Futile Recanalization Therapies in Patients With Acute Ischemic Stroke
- PMID: 35803722
- PMCID: PMC9519255
- DOI: 10.1212/WNL.0000000000200815
Multivariable Prediction Model for Futile Recanalization Therapies in Patients With Acute Ischemic Stroke
Abstract
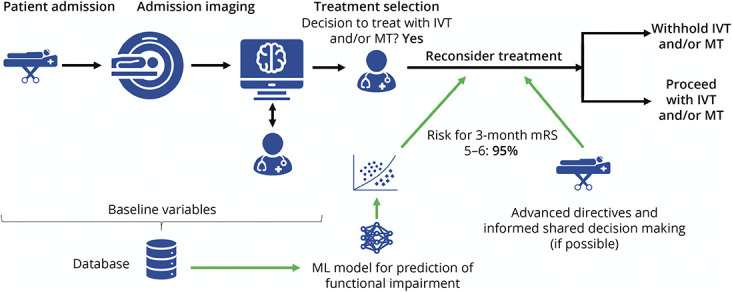
Background and objectives: Very poor outcome despite IV thrombolysis (IVT) and mechanical thrombectomy (MT) occurs in approximately 1 of 4 patients with ischemic stroke and is associated with a high logistic and economic burden. We aimed to develop and validate a multivariable prognostic model to identify futile recanalization therapies (FRTs) in patients undergoing those therapies.
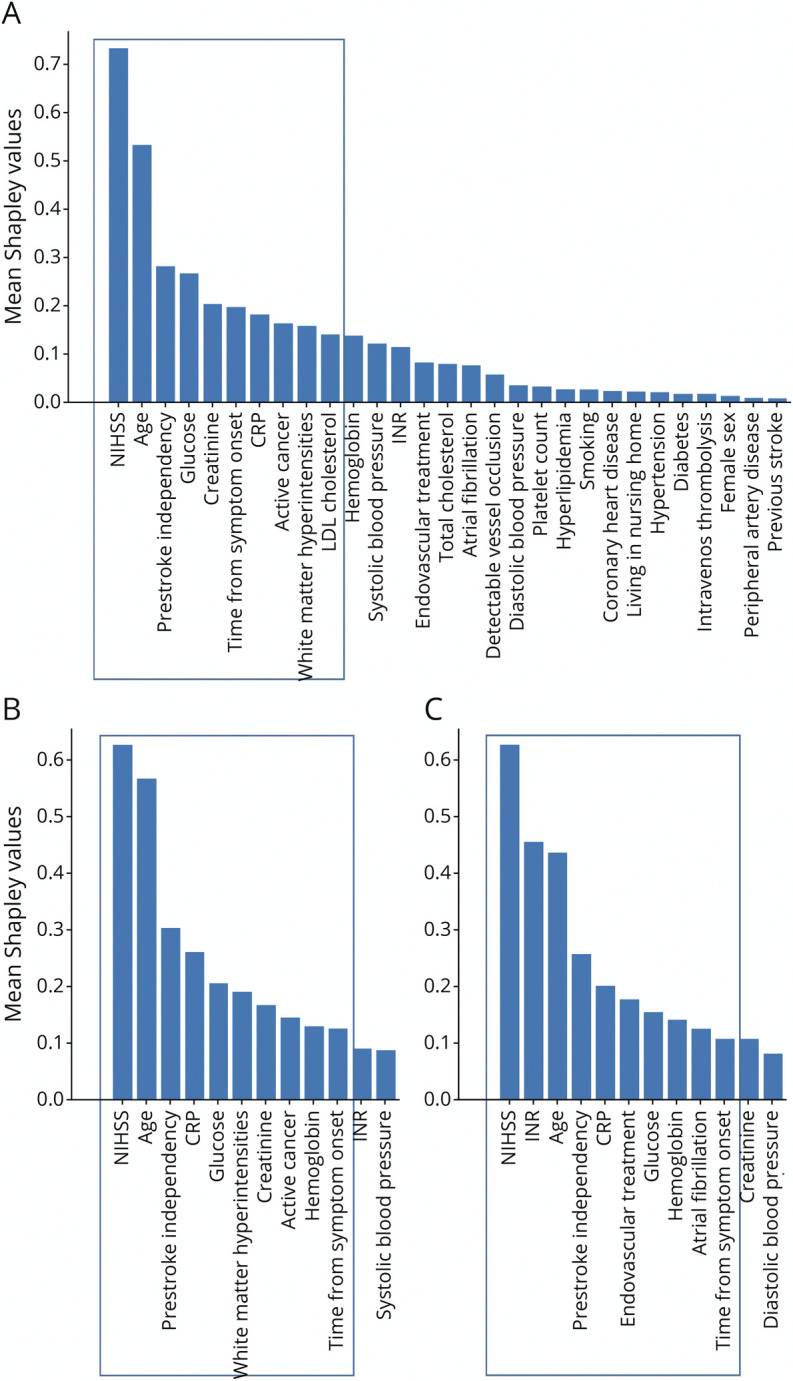
Methods: Patients from a prospectively collected observational registry of a single academic stroke center treated with MT and/or IVT were included. The data set was split into a training (N = 1,808, 80%) and internal validation (N = 453, 20%) cohort. We used gradient boosted decision tree machine learning models after k-nearest neighbor imputation of 32 variables available at admission to predict FRT defined as modified Rankin scale 5-6 at 3 months. We report feature importance, ability for discrimination, calibration, and decision curve analysis.
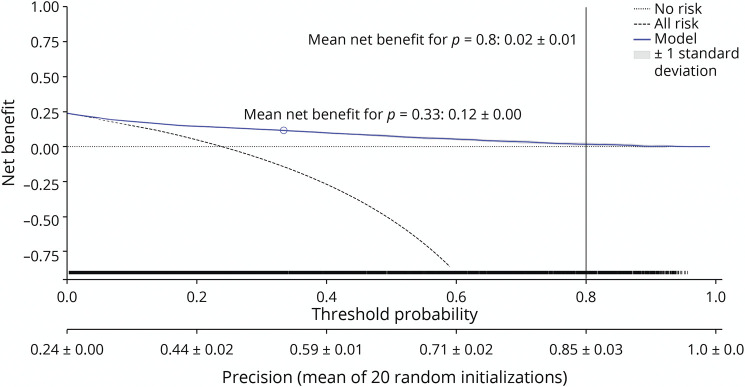
Results: A total of 2,261 patients with a median (interquartile range) age of 75 years (64-83 years), 46% female, median NIH Stroke Scale 9 (4-17), 34% IVT alone, 41% MT alone, and 25% bridging were included. Overall, 539 (24%) had FRT, more often in MT alone (34%) as compared with IVT alone (11%). Feature importance identified clinical variables (stroke severity, age, active cancer, prestroke disability), laboratory values (glucose, C-reactive protein, creatinine), imaging biomarkers (white matter hyperintensities), and onset-to-admission time as the most important predictors. The final model was discriminatory for predicting 3-month FRT (area under the curve 0.87, 95% CI 0.87-0.88) and had good calibration (Brier 0.12, 0.11-0.12). Overall performance was moderate (F1-score 0.63 ± 0.004), and decision curve analyses suggested higher mean net benefit at lower thresholds of treatment (up to 0.8).
Conclusions: This FRT prediction model can help inform shared decision making and identify the most relevant features in the emergency setting. Although it might be particularly useful in low resource healthcare settings, incorporation of further multifaceted variables is necessary to further increase the predictive performance.
Copyright © 2022 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the American Academy of Neurology.
Figures
References
-
- Ganesh A, Al-Ajlan FS, Sabiq F, et al. . Infarct in a new territory after treatment administration in the ESCAPE randomized controlled trial (endovascular treatment for small core and anterior circulation proximal occlusion with emphasis on minimizing CT to recanalization times). Stroke. 2016;47(12):2993-2998. doi:10.1161/STROKEAHA.116.014852. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials