

Mannose-binding lectin does not explain the dismal prognosis after an acute coronary event in dysglycaemic patients. A report from the GAMI cohort
- PMID: 35804351
- PMCID: PMC9270763
- DOI: 10.1186/s12933-022-01562-0
Mannose-binding lectin does not explain the dismal prognosis after an acute coronary event in dysglycaemic patients. A report from the GAMI cohort
Abstract
Background: Mannose binding lectin (MBL) has been suggested to be associated with an impaired cardiovascular prognosis in dysglycaemic conditions, but results are still contrasting. Our aims are (i) to examine whether MBL levels differ between patients with an acute myocardial infarction (MI) and healthy controls and between subgroups with different glucose tolerance status, and (ii) to investigate the relation between MBL and future cardiovascular events.
Methods: MBL levels were assessed at discharge and after 3 months in 161 AMI patients without any previously known glucose perturbations and in 183 age- and gender-matched controls from the Glucose metabolism in patients with Acute Myocardial Infarction (GAMI) study. Participants were classified as having dysglycaemia, i.e. type 2 diabetes or impaired glucose tolerance, or not by an oral glucose tolerance test. The primary outcome was a composite of cardiovascular events comprising cardiovascular death, AMI, stroke or severe heart failure during 11 years of follow-up. Total and cardiovascular mortality served as secondary outcomes.
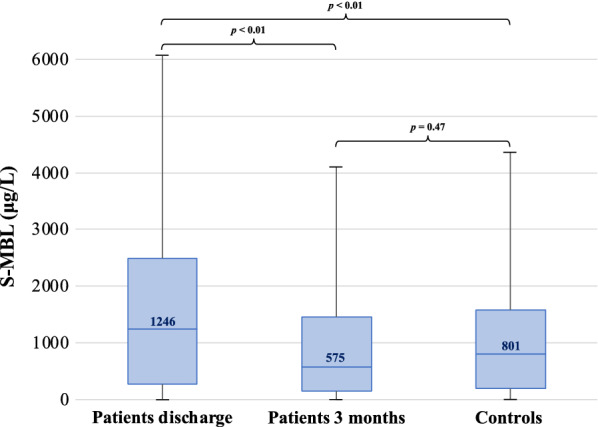
Results: At hospital discharge patients had higher MBL levels (median 1246 μg/L) than three months later (median 575 μg/L; p < 0.01), the latter did not significantly differ from those in the controls (801 μg/L; p = 0.47). MBL levels were not affected by dysglycaemia either in patients or controls. Independent of glycaemic state, increasing MBL levels did not predict any of the studied outcomes in patients. In unadjusted analyses increasing MBL levels predicted cardiovascular events (hazard ratio HR: 1.67, 95% confidence interval CI 1.06-2.64) and total mortality (HR 1.53, 95% CI 1.12-2.10) in the control group. However, this did not remain in adjusted analyses.
Conclusions: Patients had higher MBL levels than controls during the hospital phase of AMI, supporting the assumption that elevated MBL reflects acute stress. MBL was not found to be independently associated with cardiovascular prognosis in patients with AMI regardless of glucose state.
Keywords: Biomarker; Cardiovascular disease; Complement system proteins; Dysglycaemia; Inflammation; Mannose binding lectin; Prognosis.
© 2022. The Author(s).
Conflict of interest statement
The authors have no competing interests related to this work.
Figures


References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
