

Robot-Assisted Minimally Invasive Esophagectomy versus Open Esophagectomy for Esophageal Cancer: A Systematic Review and Meta-Analysis
- PMID: 35804949
- PMCID: PMC9264782
- DOI: 10.3390/cancers14133177
Robot-Assisted Minimally Invasive Esophagectomy versus Open Esophagectomy for Esophageal Cancer: A Systematic Review and Meta-Analysis
Abstract
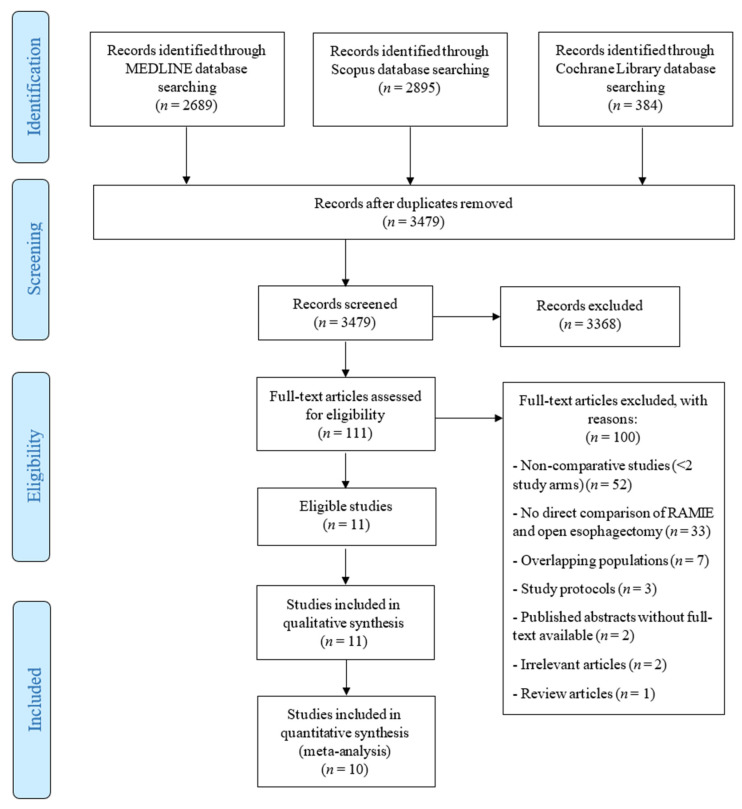
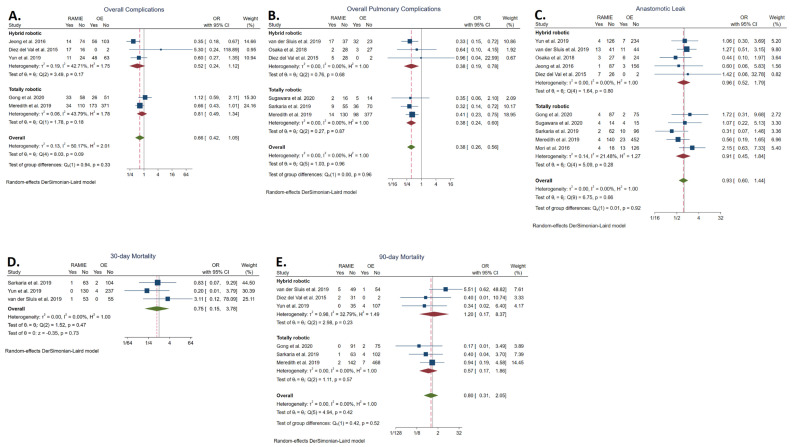
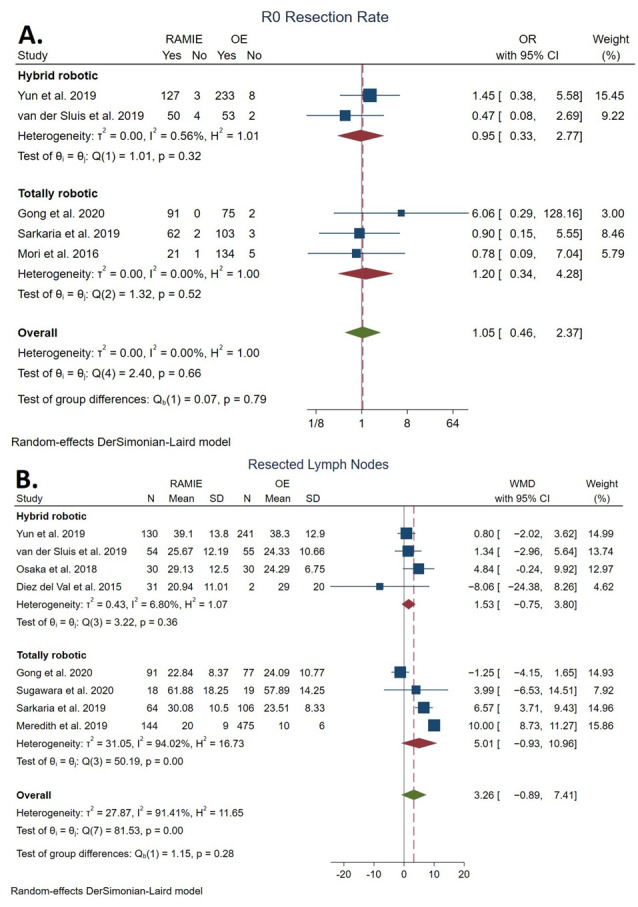
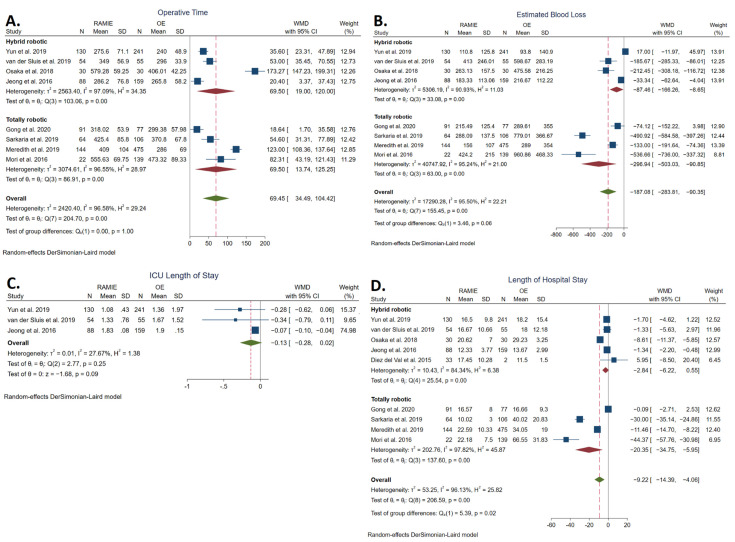
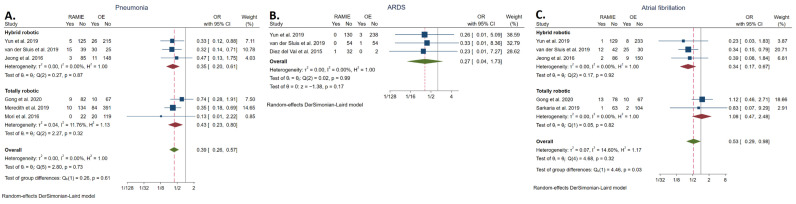
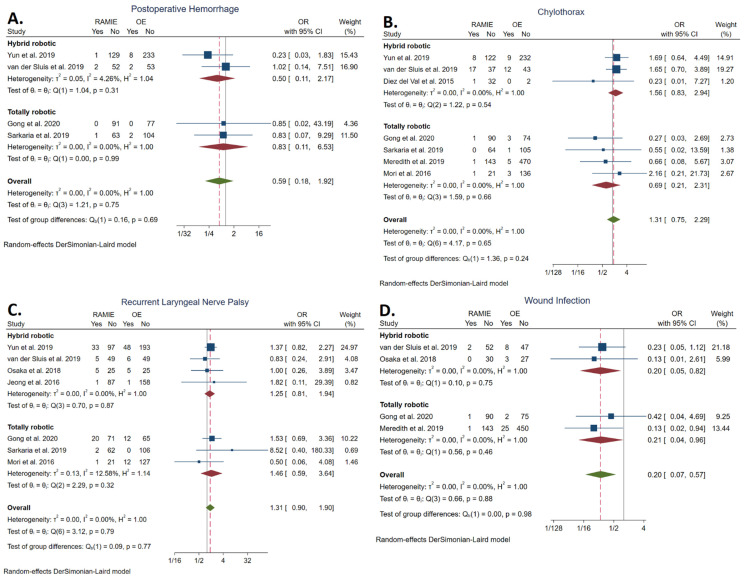
Robot-assisted minimally invasive esophagectomy (RAMIE) was introduced as a further development of the conventional minimally invasive esophagectomy, aiming to further improve the high morbidity and mortality associated with open esophagectomy. We aimed to compare the outcomes between RAMIE and open esophagectomy, which remains a popular approach for resectable esophageal cancer. Ten studies meeting our inclusion criteria were identified, including five retrospective cohort, four prospective cohort, and one randomized controlled trial. RAMIE was associated with significantly lower rates of overall pulmonary complications (odds ratio (OR): 0.38, 95% confidence interval (CI): [0.26, 0.56]), pneumonia (OR: 0.39, 95% CI: [0.26, 0.57]), atrial fibrillation (OR: 0.53, 95% CI: [0.29, 0.98]), and wound infections (OR: 0.20, 95% CI: [0.07, 0.57]) and resulted in less blood loss (weighted mean difference (WMD): -187.08 mL, 95% CI: [-283.81, -90.35]) and shorter hospital stays (WMD: -9.22 days, 95% CI: [-14.39, -4.06]) but longer operative times (WMD: 69.45 min, 95% CI: [34.39, 104.42]). No other statistically significant difference was observed regarding surgical and short-term oncological outcomes. Similar findings were observed when comparing totally robotic procedures only to OE. RAMIE is a safe and feasible procedure, resulting in decreased cardiopulmonary morbidity, wound infections, blood loss, and shorter hospital stays compared to open esophagectomy.
Keywords: RAMIE; minimally invasive esophagectomy; open esophagectomy; robot-assisted minimally invasive esophagectomy; robotic esophagectomy.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Ajani J.A., Barthel J.S., Bentrem D.J., Amico T.A.D., Das P., Denlinger C.S., Fuchs C.S., Gerdes H., Glasgow R.E., Hayman J.A., et al. Esophageal and Esophagogastric Junction Cancers Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2011;9:830–887. doi: 10.6004/jnccn.2011.0072. - DOI - PubMed
-
- Takeuchi H., Miyata H., Gotoh M., Kitagawa Y., Baba H., Kimura W., Tomita N., Nakagoe T., Shimada M., Sugihara K., et al. A Risk Model for Esophagectomy Using Data of 5354 Patients Included in a Japanese Nationwide Web-Based Database. Ann. Surg. 2014;260:259–266. doi: 10.1097/SLA.0000000000000644. - DOI - PubMed
-
- Lerut T., Moons J., Coosemans W., Van Raemdonck D., De Leyn P., Decaluwé H., Decker G., Nafteux P. Postoperative Complications after Transthoracic Esophagectomy for Cancer of the Esophagus and Gastroesophageal Junction Are Correlated with Early Cancer Recurrence: Role of Systematic Grading of Complications Using the Modified Clavien Classification. Ann. Surg. 2009;250:798–806. doi: 10.1097/SLA.0b013e3181bdd5a8. - DOI - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
