

Obstacles to Glioblastoma Treatment Two Decades after Temozolomide
- PMID: 35804976
- PMCID: PMC9265128
- DOI: 10.3390/cancers14133203
Obstacles to Glioblastoma Treatment Two Decades after Temozolomide
Abstract
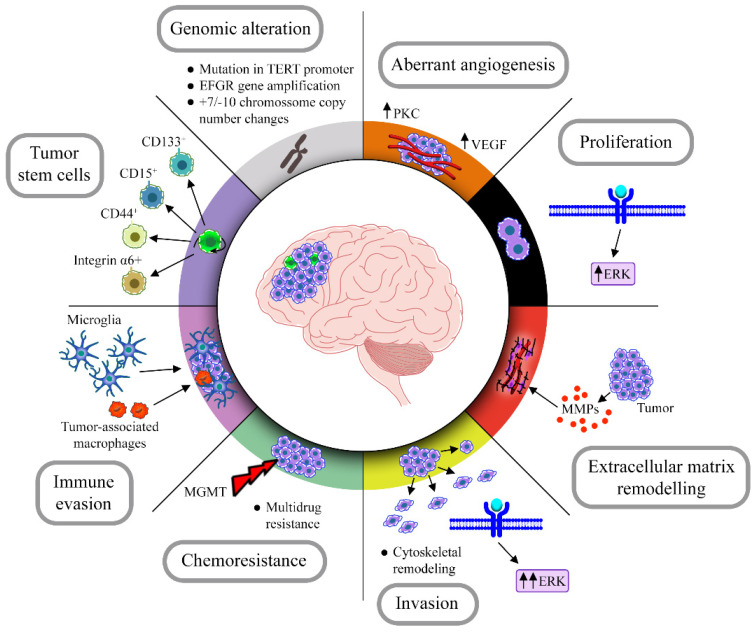
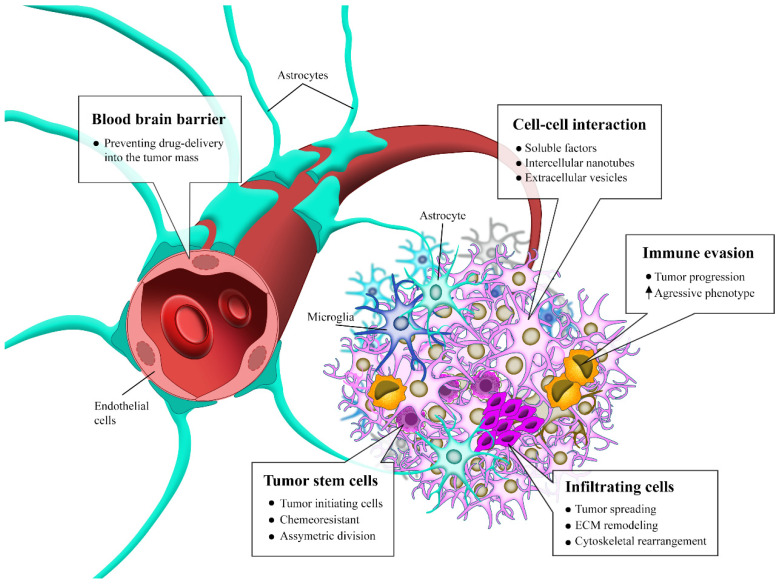
Glioblastomas are considered the most common and aggressive primary brain tumor in adults, with an average of 15 months' survival rate. The treatment is surgery resection, followed by chemotherapy with temozolomide, and/or radiotherapy. Glioblastoma must have wild-type IDH gene and some characteristics, such as TERT promoter mutation, EGFR gene amplification, microvascular proliferation, among others. Glioblastomas have great heterogeneity at cellular and molecular levels, presenting distinct phenotypes and diversified molecular signatures in each tumor mass, making it difficult to define a specific therapeutic target. It is believed that the main responsibility for the emerge of these distinct patterns lies in subcellular populations of tumor stem cells, capable of tumor initiation and asymmetric division. Studies are now focused on understanding molecular mechanisms of chemoresistance, the tumor microenvironment, due to hypoxic and necrotic areas, cytoskeleton and extracellular matrix remodeling, and in controlling blood brain barrier permeabilization to improve drug delivery. Another promising therapeutic approach is the use of oncolytic viruses that are able to destroy specifically glioblastoma cells, preserving the neural tissue around the tumor. In this review, we summarize the main biological characteristics of glioblastoma and the cutting-edge therapeutic targets that are currently under study for promising new clinical trials.
Keywords: brain tumor; cancer stem cells; chemoresistance; glioblastoma; molecular oncology.
Conflict of interest statement
João Victor Roza Cruz, Carolina Batista, Bernardo de Holanda Afonso, Magna Suzana Alexandre-Moreira, Luiz Gustavo Dubois, Bruno Pontes, Vivaldo Moura Neto and Fabio de Almeida Mendes declare no conflict of interest.
Figures
References
-
- Ostrom Q., Gittleman H., Liao P., Rouse C., Chen Y., Dowling J., Wolinsky Y., Kruchko C., Barnholtz-Sloan J. CBTRUS Statistical Report: Primary Brain and Central Nervous System Tumors Diagnosed in the United States in 2007–2011. Neuro-Oncology. 2014;16:iv1–iv63. doi: 10.1093/neuonc/nou223. - DOI - PMC - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
