

A Multimodal Biomarker Predicts Dissemination of Bronchial Carcinoid
- PMID: 35805004
- PMCID: PMC9265109
- DOI: 10.3390/cancers14133234
A Multimodal Biomarker Predicts Dissemination of Bronchial Carcinoid
Abstract
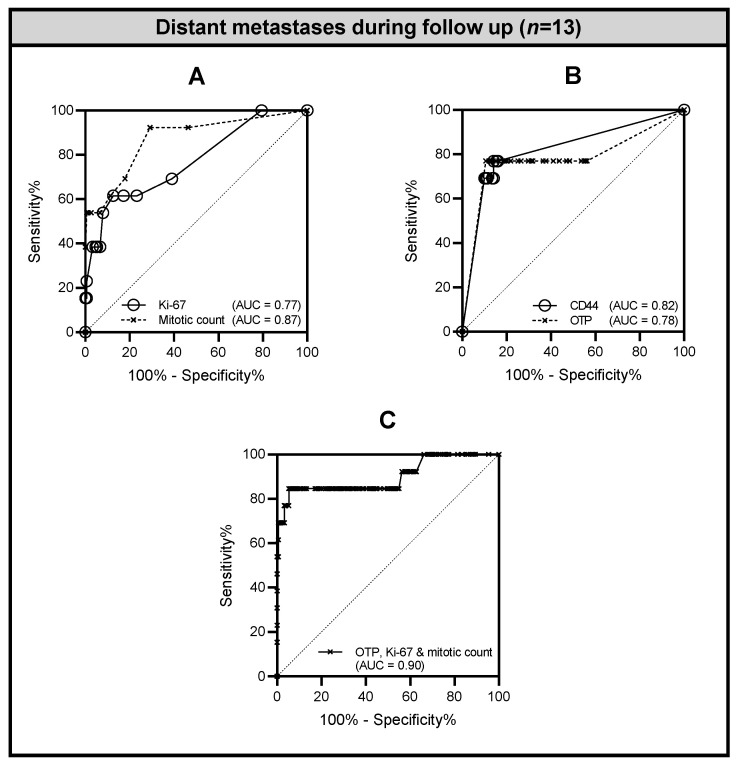
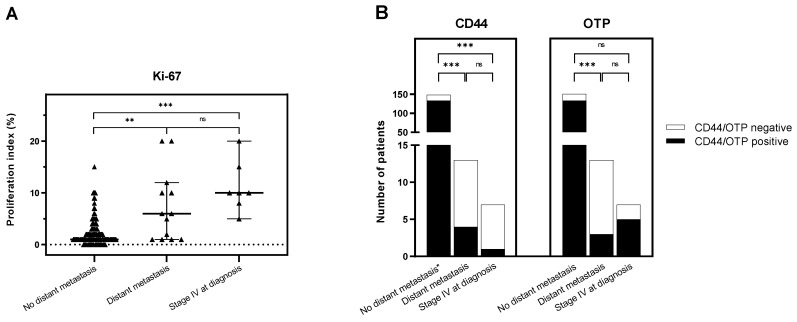
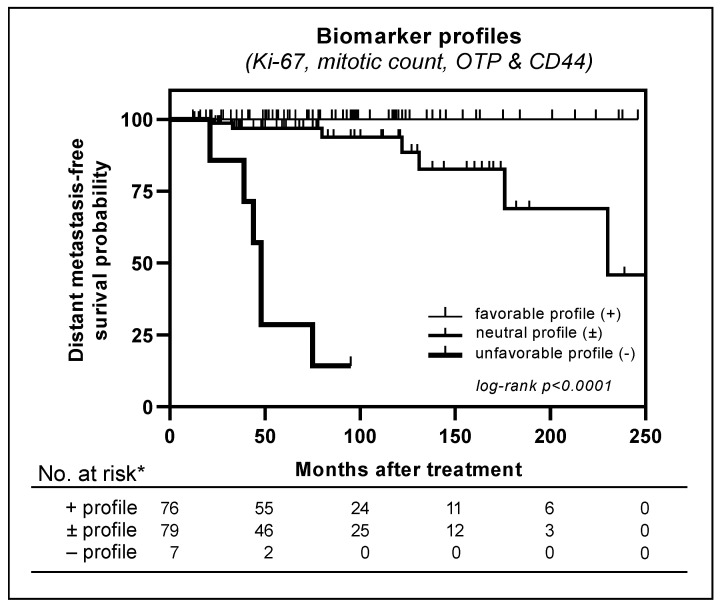
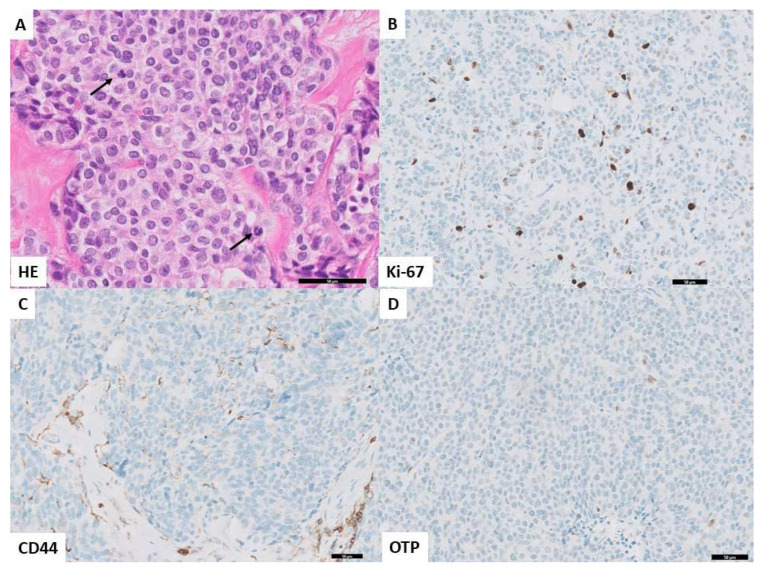
Background: Curatively treated bronchial carcinoid tumors have a relatively low metastatic potential. Gradation into typical (TC) and atypical carcinoid (AC) is limited in terms of prognostic value, resulting in yearly follow-up of all patients. We examined the additional prognostic value of novel immunohistochemical (IHC) markers to current gradation of carcinoids. Methods: A retrospective single-institution cohort study was performed on 171 patients with pathologically diagnosed bronchial carcinoid (median follow-up: 66 months). The risk of developing distant metastases based on histopathological characteristics (Ki-67, p16, Rb, OTP, CD44, and tumor diameter) was evaluated using multivariate regression analysis and the Kaplan−Meier method. Results: Of 171 patients, seven (4%) had disseminated disease at presentation, and 164 (96%) received curative-intent treatment with either endobronchial treatment (EBT) (n = 61, 36%) or surgery (n = 103, 60%). Among the 164 patients, 13 developed metastases at follow-up of 81 months (IQR 45−162). Univariate analysis showed that Ki-67, mitotic index, OTP, CD44, and tumor diameter were associated with development of distant metastases. Multivariate analysis showed that mitotic count, Ki-67, and OTP were independent risk factors for development of distant metastases. Using a 5% cutoff for Ki-67, Kaplan−Meier analysis showed that the risk of distant metastasis development was significantly associated with the number of risk predictors (AC, Ki-67 ≥ 5%, and loss of OTP or CD44) (p < 0.0001). Six out of seven patients (86%) with all three positive risk factors developed distant metastasis. Conclusions: Mitotic count, proliferation index, and OTP IHC were independent predictors of dissemination at follow-up. In addition to the widely used carcinoid classification, a comprehensive analysis of histopathological variables including Ki-67, OTP, and CD44 could assist in the determination of distant metastasis risks of bronchial carcinoids.
Keywords: Ki-67; distant metastases; immunohistochemistry; prognosis; pulmonary carcinoid.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
CD44 and OTP are strong prognostic markers for pulmonary carcinoids.Clin Cancer Res. 2013 Apr 15;19(8):2197-207. doi: 10.1158/1078-0432.CCR-12-3078. Epub 2013 Feb 26. Clin Cancer Res. 2013. PMID: 23444222
-
OTP, CD44, and Ki-67: A Prognostic Marker Panel for Relapse-Free Survival in Patients with Surgically Resected Pulmonary Carcinoid.Mod Pathol. 2025 Mar;38(3):100677. doi: 10.1016/j.modpat.2024.100677. Epub 2024 Dec 2. Mod Pathol. 2025. PMID: 39631518
-
Orthopedia Homeobox (OTP) in Pulmonary Neuroendocrine Tumors: The Diagnostic Value and Possible Molecular Interactions.Cancers (Basel). 2019 Oct 8;11(10):1508. doi: 10.3390/cancers11101508. Cancers (Basel). 2019. PMID: 31597385 Free PMC article. Review.
-
Lung carcinoid tumours: histology and Ki-67, the eternal rivalry.Histopathology. 2023 Jan;82(2):324-339. doi: 10.1111/his.14819. Epub 2022 Oct 26. Histopathology. 2023. PMID: 36239545 Free PMC article.
-
[Bronchopulmonary carcinoid tumours].Minerva Chir. 2002 Aug;57(4):403-23. Minerva Chir. 2002. PMID: 12145571 Review. Italian.
Cited by
-
Orthopedia homeobox protein (OTP) in the diagnostic and prognostic workup of pulmonary carcinoid tumors.Transl Lung Cancer Res. 2023 Jan 31;12(1):1-5. doi: 10.21037/tlcr-22-861. Epub 2022 Dec 26. Transl Lung Cancer Res. 2023. PMID: 36762060 Free PMC article. No abstract available.
-
Absence of orthopaedia homeobox protein (OTP) expression is associated with disease spread and adverse outcome in pulmonary carcinoid tumour patients.Virchows Arch. 2025 Apr;486(4):675-685. doi: 10.1007/s00428-024-03847-z. Epub 2024 Jun 19. Virchows Arch. 2025. PMID: 38896236 Free PMC article.
-
Clinical needs and pathology's answers in neuroendocrine neoplasms of the lung.Pathologica. 2025 Jun;117(3):220-242. doi: 10.32074/1591-951X-N1102. Epub 2025 Jun 27. Pathologica. 2025. PMID: 40574629 Free PMC article. Review.
-
Differential Orthopedia Homeobox expression in pulmonary carcinoids is associated with changes in DNA methylation.Int J Cancer. 2022 Jun 15;150(12):1987-1997. doi: 10.1002/ijc.33939. Epub 2022 Feb 16. Int J Cancer. 2022. PMID: 35076935 Free PMC article.
References
-
- WHO Classification of Tumours. 5th ed. WHO; Geneva, Switzerland: 2021. Thoracic Tumours.
LinkOut - more resources
Full Text Sources
Miscellaneous
