

Identification of growth hormone receptor as a relevant target for precision medicine in low-EGFR expressing glioblastoma
- PMID: 35808822
- PMCID: PMC9270581
- DOI: 10.1002/ctm2.939
Identification of growth hormone receptor as a relevant target for precision medicine in low-EGFR expressing glioblastoma
Abstract
Objective: New therapeutic approaches are needed to improve the prognosis of glioblastoma (GBM) patients.
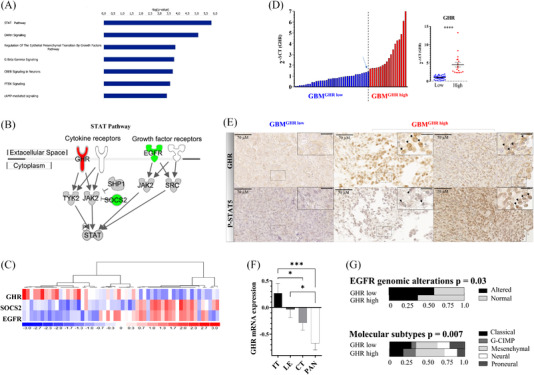
Methods: With the objective of identifying alternative oncogenic mechanisms to abnormally activated epidermal growth factor receptor (EGFR) signalling, one of the most common oncogenic mechanisms in GBM, we performed a comparative analysis of gene expression profiles in a series of 54 human GBM samples. We then conducted gain of function as well as genetic and pharmocological inhibition assays in GBM patient-derived cell lines to functionnally validate our finding.
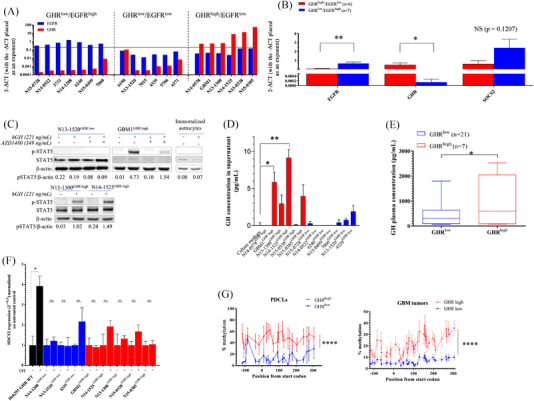
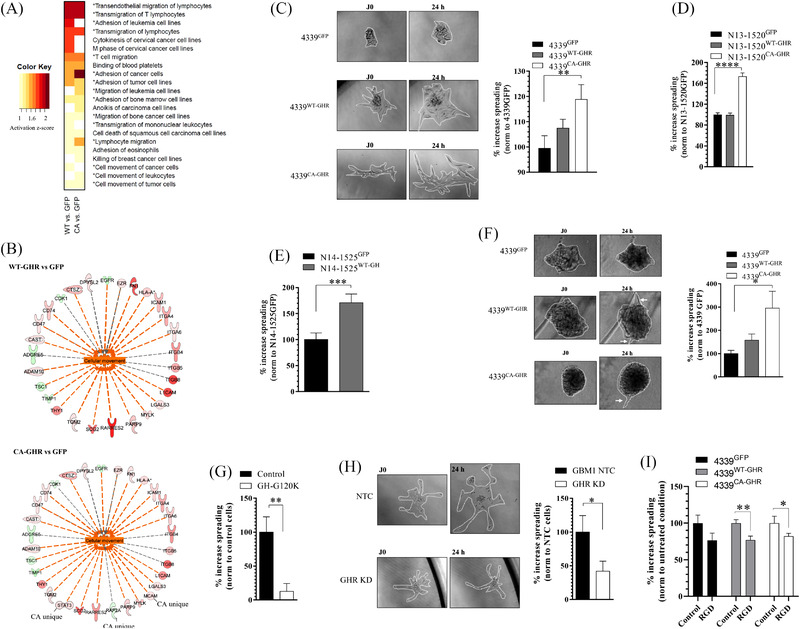
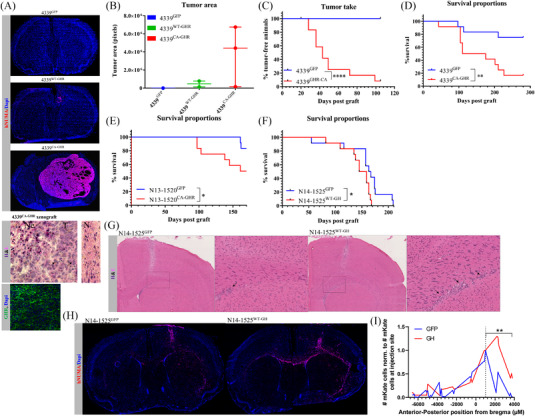
Results: We identified that growth hormone receptor (GHR) signalling defines a distinct molecular subset of GBMs devoid of EGFR overexpression. GHR overexpression was detected in one third of patients and was associated with low levels of suppressor of cytokine signalling 2 (SOCS2) expression due to SOCS2 promoter hypermethylation. In GBM patient-derived cell lines, GHR signalling modulates the expression of proteins involved in cellular movement, promotes cell migration, invasion and proliferation in vitro and promotes tumourigenesis, tumour growth, and tumour invasion in vivo. GHR genetic and pharmacological inhibition reduced cell proliferation and migration in vitro.
Conclusion: This study pioneers a new field of investigation to improve the prognosis of GBM patients.
Keywords: cell migration; comparative analysis; glioblastoma; oncogenicity; pre-clinical models; therapeutic target; tumour invasion.
© 2022 The Authors. Clinical and Translational Medicine published by John Wiley & Sons Australia, Ltd on behalf of Shanghai Institute of Clinical Bioinformatics.
Conflict of interest statement
The authors declare that there is no conflict of interest that could be perceived as prejudicing the impartiality of the research reported.
Figures

References
-
- Hess KR, Broglio KR, Bondy ML. Adult glioma incidence trends in the United States, 1977–2000. Cancer. 2004;101:2293‐2299. - PubMed
-
- Bauchet L, Rigau V, Mathieu‐Daude H, et al. French brain tumor data bank: methodology and first results on 10,000 cases. J Neurooncol. 2007;84:189‐199. - PubMed
-
- Stupp R, Mason WP, van den Bent MJ, et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med. 2005;352:987‐996. - PubMed
-
- Keime‐Guibert F, Chinot O, Taillandier L, et al.; Association of French‐Speaking Neuro‐Oncologists . Radiotherapy for glioblastoma in the elderly. N Engl J Med. 2007;356:1527‐1535. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources