

α-Synuclein Seed Amplification in CSF and Brain from Patients with Different Brain Distributions of Pathological α-Synuclein in the Context of Co-Pathology and Non-LBD Diagnoses
- PMID: 35808984
- PMCID: PMC9489647
- DOI: 10.1002/ana.26453
α-Synuclein Seed Amplification in CSF and Brain from Patients with Different Brain Distributions of Pathological α-Synuclein in the Context of Co-Pathology and Non-LBD Diagnoses
Abstract
Objective: The purpose of this study was to determine the sensitivity and specificity of α-synuclein seed amplification assay (αSyn-SAA) in antemortem and postmortem cerebrospinal fluid (CSF) of autopsy-confirmed patients with different distributions of pathological αSyn, co-pathologies, and clinical diagnoses.
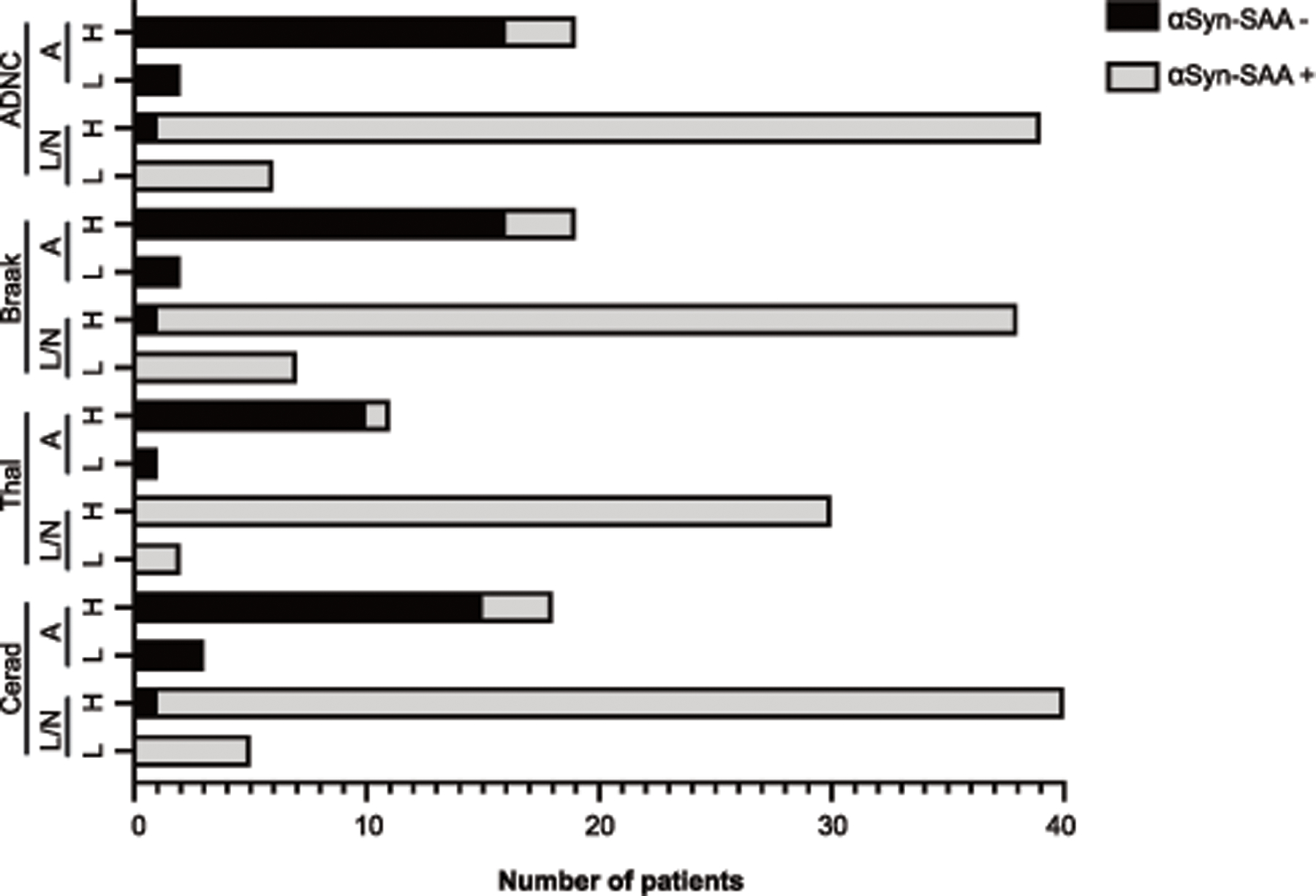
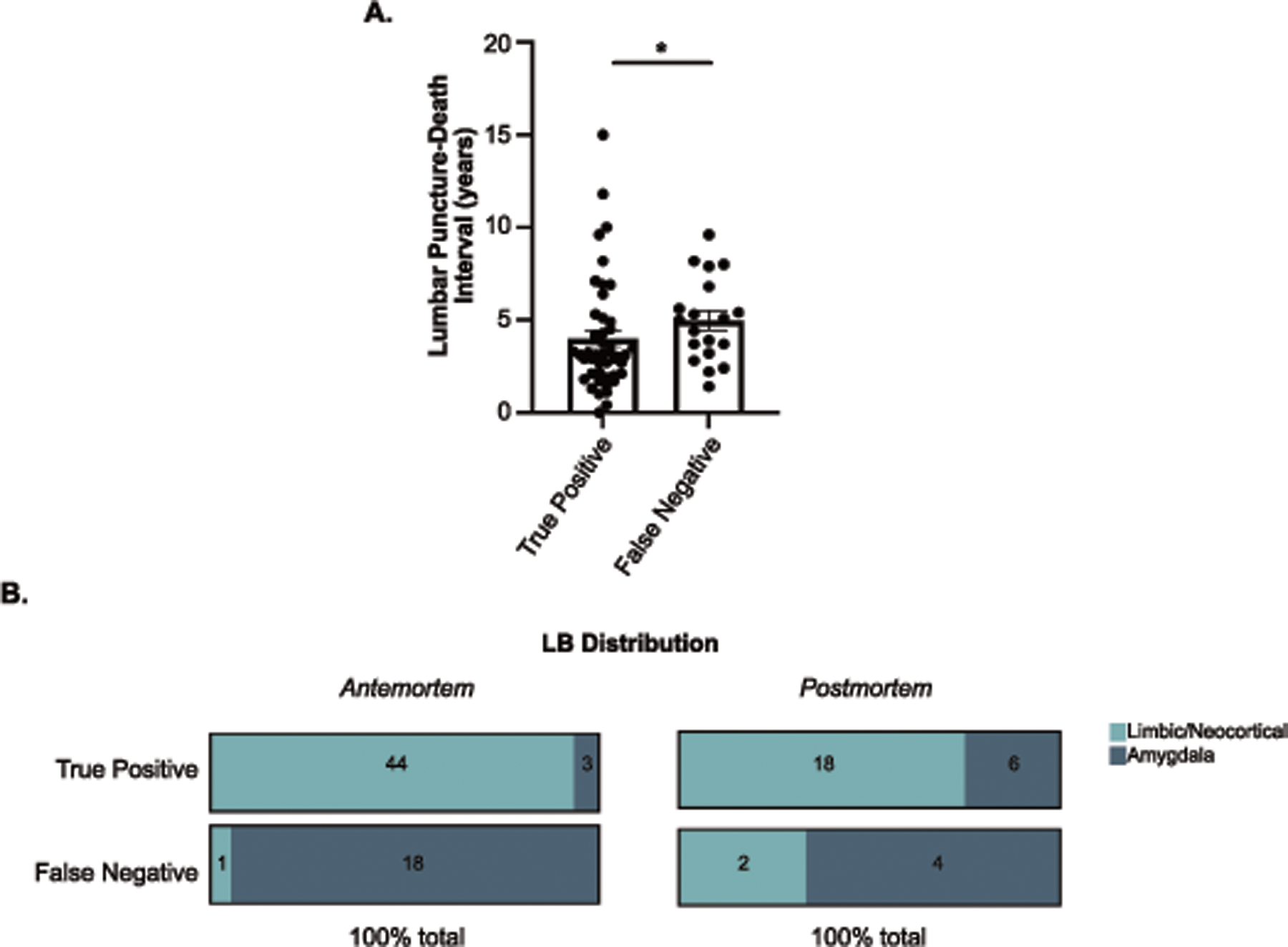
Methods: The αSyn-SAA was used to test antemortem CSF samples from 119 subjects with a variety of clinical syndromes and standardized neuropathological examinations from Oregon Health and Science University (OHSU) and University of California San Diego (UCSD; 56 additional postmortem CSF samples available). The αSyn-SAA was also applied to frontal cortex and amygdala homogenates. Sensitivity and specificity were compared across distributions of αSyn pathology. Clinical data and co-pathologies were compared across αSyn-SAA positive and negative groups.
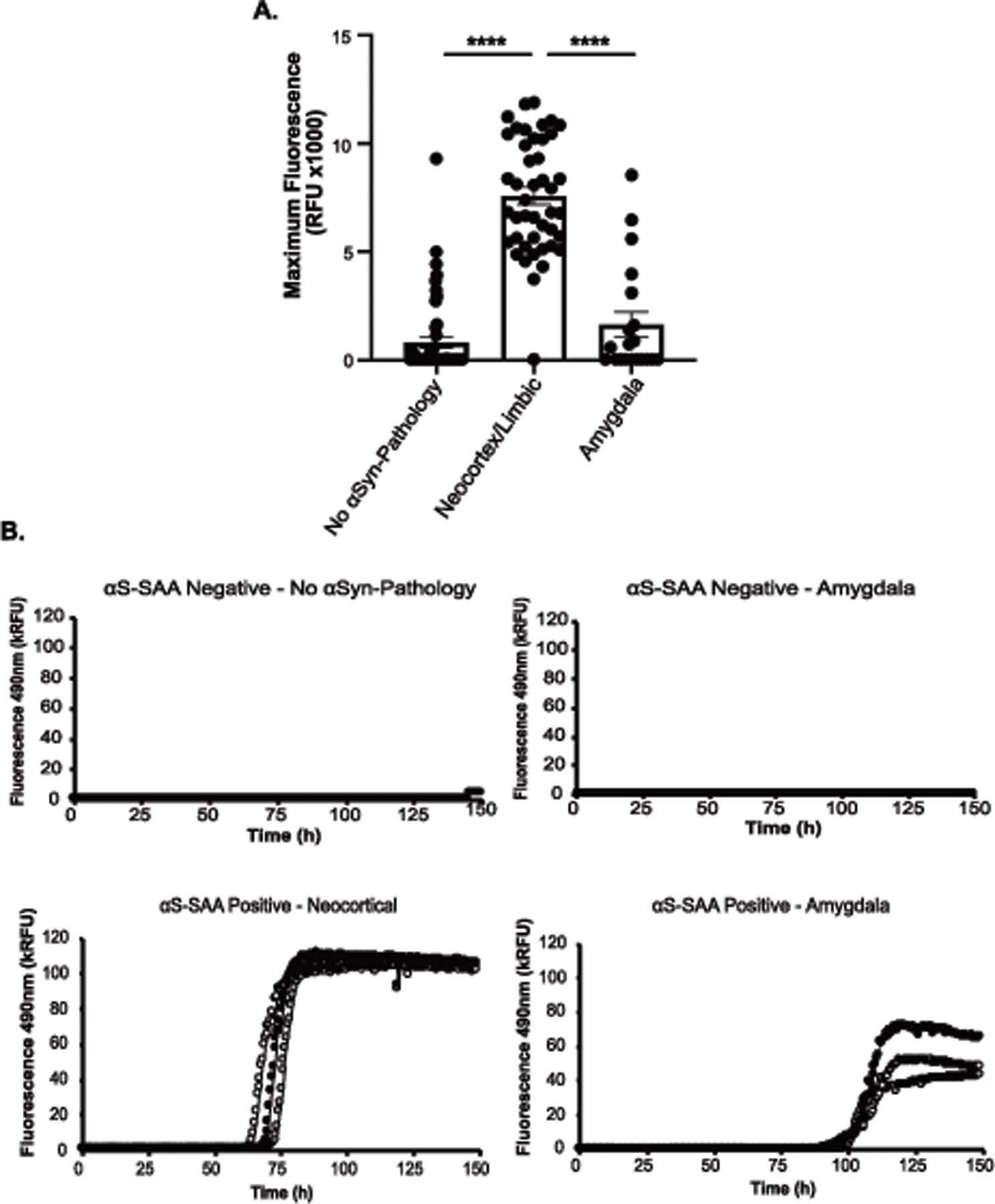
Results: Fifty-three individuals without and 66 with αSyn-pathology (neocortical [n = 38], limbic [n = 7], and amygdala-predominant [n = 21]) were included. There was a sensitivity of 97.8% and specificity of 98.1% of the αSyn-SAA to identify patients with limbic/neocortical pathology from antemortem CSF. Sensitivity to detect amygdala-predominant pathology was only 14.3%. Postmortem CSF and brain tissue αSyn-SAA analyses also showed higher assay positivity in samples from limbic/neocortical cases.
Interpretation: CSF αSyn-SAA reliably identifies αSyn seeds in patients with diffuse αSyn pathology in the context of co-pathology and non-Lewy body disease (LBD) diagnoses. The analysis of brain homogenates suggests that pathological αSyn in the amygdala might differ from pathological αSyn in the frontal cortex. The αSyn-SAA might facilitate the differential diagnosis of dementias with mixed pathologies. ANN NEUROL 2022;92:650-662.
© 2022 American Neurological Association.
Conflict of interest statement
Potential Conflicts of Interest
Dr. Concha, Ms. Farris, and Mr. Ma are inventors on several patents related to PMCA technology (SAA) and are associated to Amprion Inc, a biotech company focused on the commercial utilization of SAA for diagnosis. All other authors have no conflicts of interest to disclose.
Figures
References
-
- Jellinger KA. Alpha-synuclein pathology in Parkinson’s and Alzheimer’s disease brain: incidence and topographic distribution--a pilot study. Acta Neuropathol 2003; 106 (3): 191–201. - PubMed
-
- Kotzbauer PT, Trojanowsk JQ, Lee VM. Lewy body pathology in Alzheimer’s disease. J Mol Neurosci 2001; 17 (2): 225–232. - PubMed
