

Gastrointestinal stromal tumors: a comprehensive radiological review
- PMID: 35809209
- PMCID: PMC9616766
- DOI: 10.1007/s11604-022-01305-x
Gastrointestinal stromal tumors: a comprehensive radiological review
Abstract
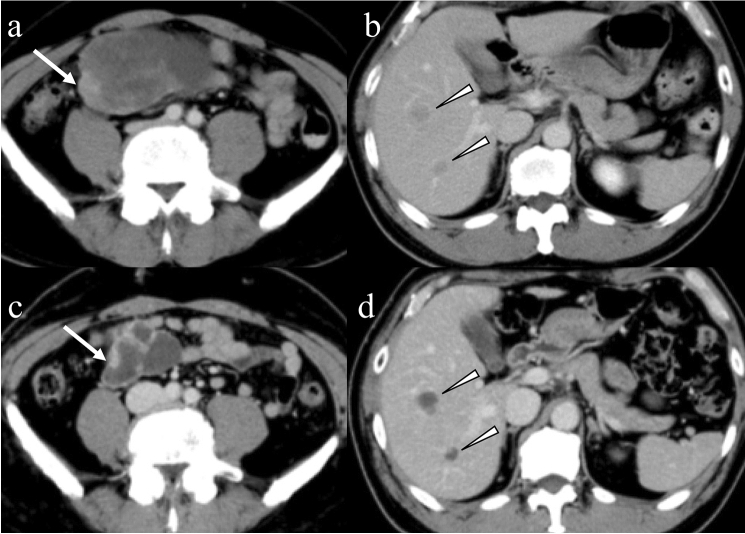
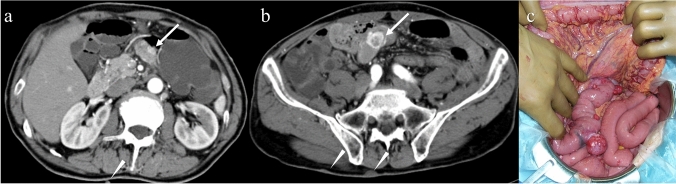
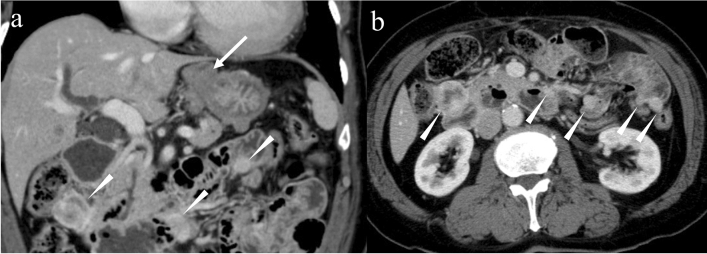
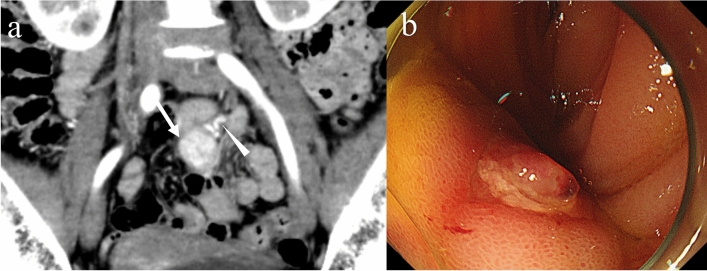
Gastrointestinal stromal tumors (GISTs) originating from the interstitial cells of Cajal in the muscularis propria are the most common mesenchymal tumor of the gastrointestinal tract. Multiple modalities, including computed tomography (CT), magnetic resonance imaging (MRI), fluorodeoxyglucose positron emission tomography, ultrasonography, digital subtraction angiography, and endoscopy, have been performed to evaluate GISTs. CT is most frequently used for diagnosis, staging, surveillance, and response monitoring during molecularly targeted therapy in clinical practice. The diagnosis of GISTs is sometimes challenging because of the diverse imaging findings, such as anatomical location (esophagus, stomach, duodenum, small bowel, colorectum, appendix, and peritoneum), growth pattern, and enhancement pattern as well as the presence of necrosis, calcification, ulceration, early venous return, and metastasis. Imaging findings of GISTs treated with antineoplastic agents are quite different from those of other neoplasms (e.g. adenocarcinomas) because only subtle changes in size are seen even in responsive lesions. Furthermore, the recurrence pattern of GISTs is different from that of other neoplasms. This review discusses the advantages and disadvantages of each imaging modality, describes imaging findings obtained before and after treatment, presents a few cases of complicated GISTs, and discusses recent investigations performed using CT and MRI to predict histological risk grade, gene mutations, and patient outcomes.
Keywords: Acute abdomen; Gastrointestinal stromal tumors; Magnetic resonance imaging; Multidetector computed tomography; Proto-oncogene proteins c-kit.
© 2022. The Author(s).
Conflict of interest statement
No potential conflict of interest was reported by the authors.
Figures

References
-
- Joensuu H, Hohenberger P, Corless CL. Gastrointestinal stromal tumour. The Lancet. 2013;382(9896):973–983. - PubMed
-
- Yan J, Zhao X, Han S, Wang T, Miao F. Evaluation of clinical plus imaging features and multidetector computed tomography texture analysis in preoperative risk grade prediction of small bowel gastrointestinal stromal tumors. J Comput Assist Tomogr. 2018;42(5):714–720. - PubMed
-
- Xu F, Ma X, Wang Y, Tian Y, Tang W, Wang M, et al. CT texture analysis can be a potential tool to differentiate gastrointestinal stromal tumors without KIT exon 11 mutation. Eur J Radiol. 2018;107:90–97. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
