

Estimates, trends, and drivers of the global burden of type 2 diabetes attributable to PM2·5 air pollution, 1990-2019: an analysis of data from the Global Burden of Disease Study 2019
- PMID: 35809588
- PMCID: PMC9278144
- DOI: 10.1016/S2542-5196(22)00122-X
Estimates, trends, and drivers of the global burden of type 2 diabetes attributable to PM2·5 air pollution, 1990-2019: an analysis of data from the Global Burden of Disease Study 2019
Abstract
Background: Experimental and epidemiological studies indicate an association between exposure to particulate matter (PM) air pollution and increased risk of type 2 diabetes. In view of the high and increasing prevalence of diabetes, we aimed to quantify the burden of type 2 diabetes attributable to PM2·5 originating from ambient and household air pollution.
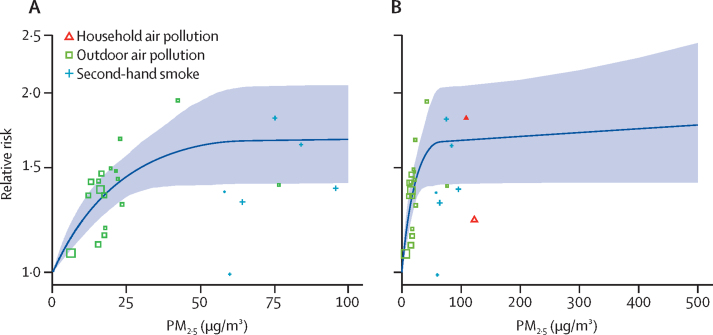
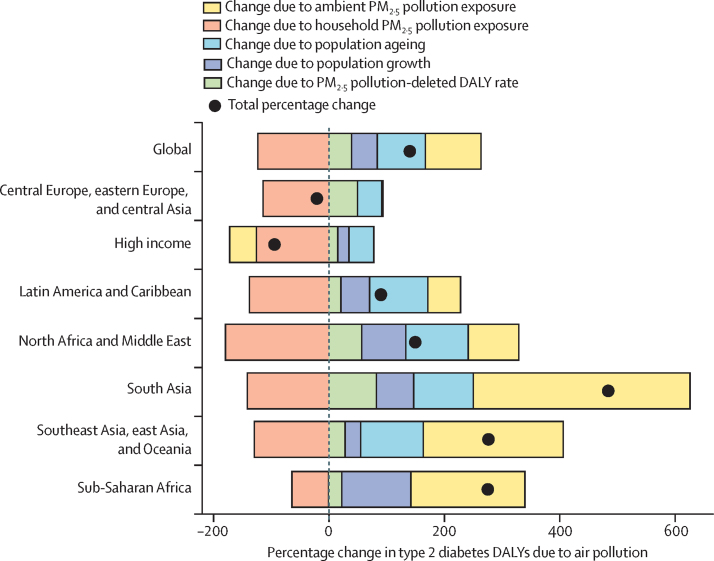
Methods: We systematically compiled all relevant cohort and case-control studies assessing the effect of exposure to household and ambient fine particulate matter (PM2·5) air pollution on type 2 diabetes incidence and mortality. We derived an exposure-response curve from the extracted relative risk estimates using the MR-BRT (meta-regression-Bayesian, regularised, trimmed) tool. The estimated curve was linked to ambient and household PM2·5 exposures from the Global Burden of Diseases, Injuries, and Risk Factors Study 2019, and estimates of the attributable burden (population attributable fractions and rates per 100 000 population of deaths and disability-adjusted life-years) for 204 countries from 1990 to 2019 were calculated. We also assessed the role of changes in exposure, population size, age, and type 2 diabetes incidence in the observed trend in PM2·5-attributable type 2 diabetes burden. All estimates are presented with 95% uncertainty intervals.
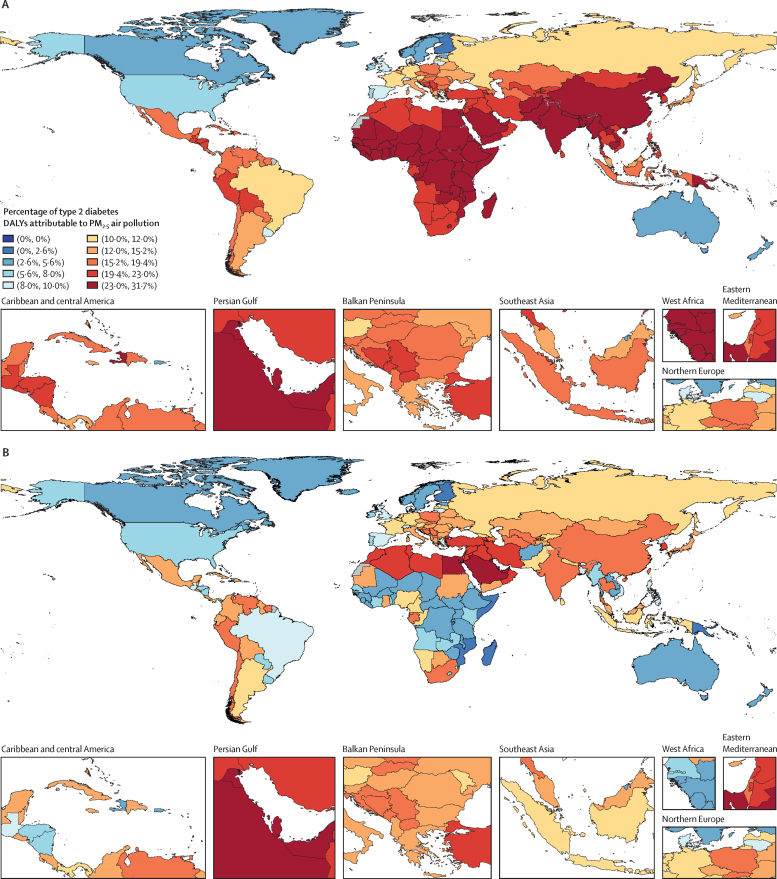
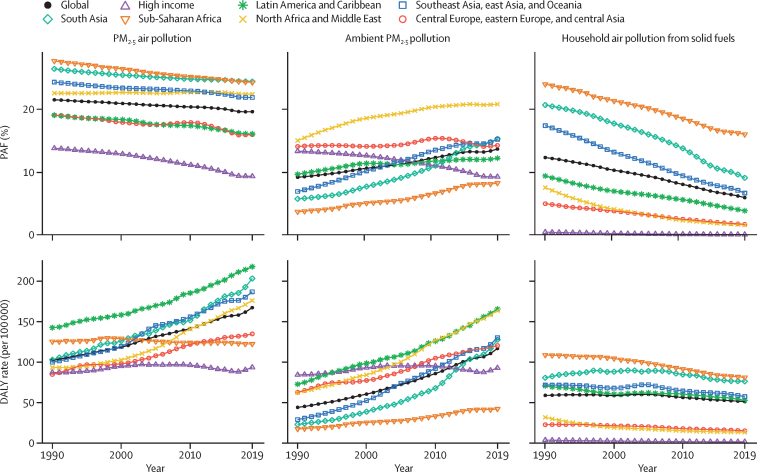
Findings: In 2019, approximately a fifth of the global burden of type 2 diabetes was attributable to PM2·5 exposure, with an estimated 3·78 (95% uncertainty interval 2·68-4·83) deaths per 100 000 population and 167 (117-223) disability-adjusted life-years (DALYs) per 100 000 population. Approximately 13·4% (9·49-17·5) of deaths and 13·6% (9·73-17·9) of DALYs due to type 2 diabetes were contributed by ambient PM2·5, and 6·50% (4·22-9·53) of deaths and 5·92% (3·81-8·64) of DALYs by household air pollution. High burdens, in terms of numbers as well as rates, were estimated in Asia, sub-Saharan Africa, and South America. Since 1990, the attributable burden has increased by 50%, driven largely by population growth and ageing. Globally, the impact of reductions in household air pollution was largely offset by increased ambient PM2·5.
Interpretation: Air pollution is a major risk factor for diabetes. We estimated that about a fifth of the global burden of type 2 diabetes is attributable PM2·5 pollution. Air pollution mitigation therefore might have an essential role in reducing the global disease burden resulting from type 2 diabetes.
Funding: Bill & Melinda Gates Foundation.
Copyright © 2022 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests T W Bärnighausen reports support for the present manuscript from the Alexander von Humboldt Foundation, Wellcome Trust, German Research Foundation, and US National Institutes of Health (National Institute of Allergy and Infectious Diseases, National Institute on Aging, and Fogarty International Center), all paid to his institution. Y Béjot reports consulting fees from Novo Nordisk and honoraria for lectures from Medtronic, Boehringer Ingelheim, Pfizer, Bristol Myers Squibb (BMS), Servier Laboratories, and Amgen, all outside the submitted work. L A Càmera reports non-financial support for the present manuscript from Sociedad Argentina de Medicina and Hospital Italiano Buenos Aires. X Dai reports support for the present manuscript via salary from the Institute for Health Metrics and Evaluation University of Washington. I Filip and A Radfar report support from Avicenna Medical and Clinical Research Institute, outside the submitted work. J J Jozwiak reports payment via personal fees for lectures, presentations, speaker's bureaus, manuscript writing or educational events from Teva Pharmaceuticals, Amgen, Synexus, Boehringer Ingelheim, Zentiva, and Sanofi, all outside the submitted work. M Kivimäki reports research grants to University College London (London, UK) from the Wellcome Trust (221854/Z/20/Z) and the UK Medical Research Council (MR/S011676/1), outside the submitted work. S Lorkowski reports (all outside the submitted work) grants or contracts paid to his institution from Akcea Therapeutics Germany; consulting fees from Danone, Novartis Pharma, Swedish Orphan Biovitrum (SOBI), and Upfield; payment or honoraria for lectures, presentations, speaker's bureaus, manuscript writing, or educational events from Akcea Therapeutics Germany, Amarin Germany, Amedes Holding, Amgen, Berlin-Chemie, Boehringer Ingelheim, Daiichi Sankyo Deutschland, Danone, Hubert Burda Media Holding, Janssen-Cilag, Lilly Deutschland, Novartis, Novo Nordisk, F Hoffmann-La Roche (Roche), Sanofi-Aventis, SYNLAB Holding Deutschland, and SYNLAB Akademie; support for attending meetings or travel from Amgen; and participation on a data safety monitoring board or advisory board for Akcea Therapeutics Germany, Amgen, Daiichi Sankyo Deutschland, Novartis, and Sanofi-Aventis. P W Mahasha reports (all outside the submitted work) participation on a data safety monitoring board or advisory board as a member of the Technical Advisory Panel to the Office of Health Standards Compliance and Health Ombud from Feb 12, 2020, to Feb 11, 2022, and leadership or fiduciary roles in boards, societies, committees, or advocacy groups, paid or unpaid, as a member of the Federation of Infectious Diseases Societies of Southern Africa since November, 2021; the EU-Africa PerMed Consortium from February, 2021, to January, 2025; the South African Society for Biochemistry and Molecular Biology since August, 2021; the International Society for Infectious Diseases since November, 2021; the South African Society of Microbiology since November, 2021; the COVID-19 Clinical Research Coalition since August, 2021; the Scholars Academic and Scientific Society since August, 2021; Cochrane International since October, 2019 (renewed on March 13, 2022); and the South African Council for Natural Scientific Professions since June, 2018. A Ortiz reports (all outside the submitted work) grants from Sanofi; consultancy or speaker fees or travel support from Advicenne, Astellas, AstraZeneca, Amicus, Amgen, Fresenius Medical Care, GlaxoSmithKline, Bayer, Sanofi-Genzyme, Menarini, Kyowa Kirin, Alexion, Idorsia, Chiesi, Otsuka, Novo-Nordisk, and Vifor Fresenius Medical Care Renal Pharma; is Director of the Catedra Mundipharma-UAM of diabetic kidney disease and the Catedra AstraZeneca-UAM of chronic kidney disease and electrolytes; is the Editor-in-Chief for Clinical Kidney Journal; and reports a leadership or fiduciary role with the European Renal Association and Madrid Renal Association. P A Mahesh reports grants or contracts paid to his institution from the Government of India (Wellcome Trust/DBT team science grant), the US National Institutes of Health Global Infectious Diseases, and the Swedish Heart Lung Foundation, outside the submitted work. M J Postma reports grants paid to his institution from Boehringer Ingelheim and AstraZeneca, and stock or stock options in Health-Ecore (25%) and Pharmacoeconomics Advice Groningen (100%), all outside the submitted work. J Sanabria reports a pending patent for pNaKtide, and leadership or fiduciary roles in boards, societies, committees, or advocacy groups, paid or unpaid with the Society for the Surgery of the Alimentary Tract, American Association for the Study of Liver Diseases, Society of University Surgeons, and American Society of Transplant Surgeons, all outside the submitted work. P R Valdez reports support for the present manuscript from Sociedad Argentina de Medicina and Hospital Velez Sarsfield Buenos Aires. All other authors declare no competing interests.
Figures

References
-
- WHO Global report on diabetes. April 21, 2016. https://www.who.int/publications/i/item/9789241565257
-
- Hotamisligil GS. Inflammation and metabolic disorders. Nature. 2006;444:860–867. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
