

Racial inequalities in multimorbidity: baseline of the Brazilian Longitudinal Study of Adult Health (ELSA-Brasil)
- PMID: 35810284
- PMCID: PMC9270815
- DOI: 10.1186/s12889-022-13715-7
Racial inequalities in multimorbidity: baseline of the Brazilian Longitudinal Study of Adult Health (ELSA-Brasil)
Abstract
Background: Evidence of multimorbidity has come mainly from high-income regions, while disparities among racial groups have been less explored. This study examined racial differences in multimorbidity in the multiracial cohort of the Longitudinal Study of Adult Health (Estudo Longitudinal de Saúde do Adulto), ELSA-Brasil.
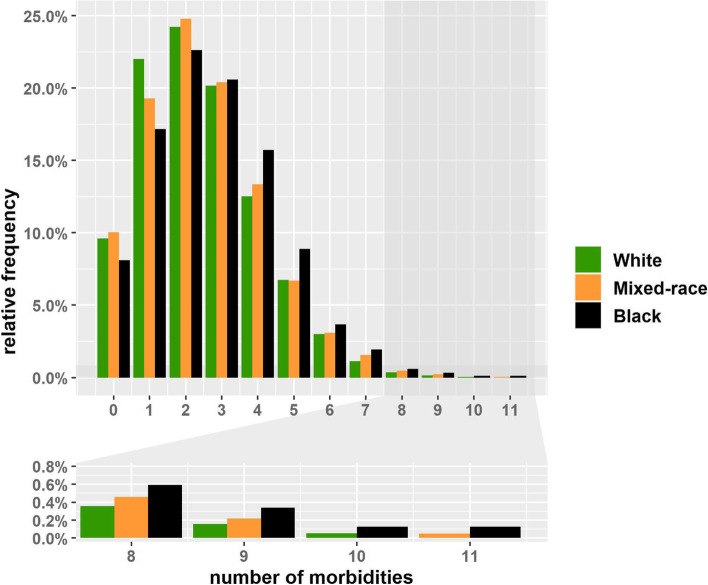
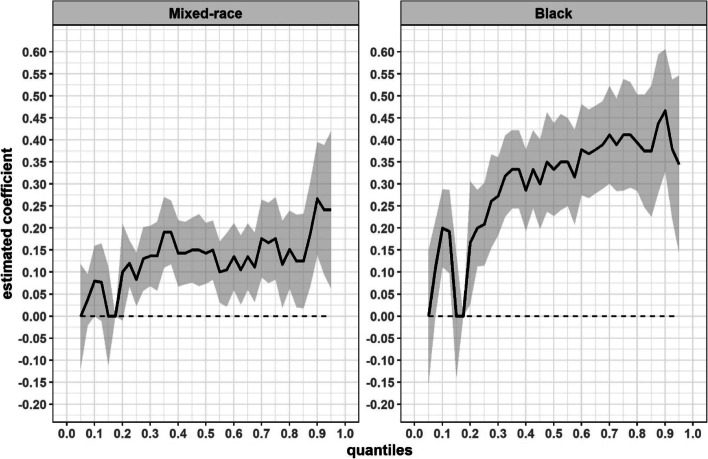
Methods: The study examined baseline (2008-2010) data for 14 099 ELSA-Brasil participants who self-reported being white, mixed-race, or black. A list of 16 morbidities was used to evaluate multimorbidity, operationalised by simple count into ≥ 2, ≥ 3, ≥ 4, ≥ 5 and ≥ 6 morbidities, in addition to evaluating the number of coexisting conditions. Prevalence ratios (PR) were estimated from logistic models and a quantile model was used to examine racial differences graphically in the distribution quantiles for the number of morbidities.
Results: Overall prevalence of multimorbidity (≥ 2 morbidities) was 70% and, after controlling for age and sex, was greater among mixed-race and black participants - by 6% (PR: 1.06; 95% CI: 1.03-1.08) and 9% (PR: 1.09; 95% CI: 1.06-1.12), respectively - than among white participants. As the cutoff value for defining multimorbidity was raised, so the strength of the association increased, especially among blacks: if set at ≥ 6 morbidities, the prevalence was 27% greater for those of mixed-race (PR: 1.27; 95% CI: 1.07-1.50) and 47% greater for blacks (PR: 1.47; 95% CI: 1.22-1.76) than for whites. The disparities were smaller in the lower morbidity distribution quantiles and larger in the upper quantiles, indicating a heavier burden of disease, particularly on blacks.
Conclusions: Multimorbidity was common among adults and older adults in a Brazilian cohort, but important racial inequalities were found. Raising the cutoff point for defining multimorbidity revealed stronger associations between race/skin colour and multimorbidity, indicating a higher prevalence of multimorbidity among mixed-race and black individuals than among whites and that the former groups coexisted more often with more complex health situations (with more coexisting morbidities). Interventions to prevent and manage the condition of multimorbidity that consider the social determinants of health and historically discriminated populations in low- and middle-income regions are necessary.
Keywords: Chronic disease; Disease accumulation; Multimorbidity; Racial inequalities in health; Social determinants of health.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- World Health Organization . Multimorbidity: Technical Series on Safer Primary Care. Geneva: World Health Organization; 2016.
-
- The Academy of Medical Sciences. Multimorbidity: a priority for global health research. 2018. Available from: https://acmedsci.ac.uk/file-download/82222577
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
