

Niraparib plus nivolumab or niraparib plus ipilimumab in patients with platinum-sensitive advanced pancreatic cancer: a randomised, phase 1b/2 trial
- PMID: 35810751
- PMCID: PMC9339497
- DOI: 10.1016/S1470-2045(22)00369-2
Niraparib plus nivolumab or niraparib plus ipilimumab in patients with platinum-sensitive advanced pancreatic cancer: a randomised, phase 1b/2 trial
Erratum in
-
Correction to Lancet Oncol 2022; 23: 1009-20.Lancet Oncol. 2022 Oct;23(10):e446. doi: 10.1016/S1470-2045(22)00571-X. Lancet Oncol. 2022. PMID: 36174629 Free PMC article. No abstract available.
Abstract
Background: Establishing alternatives to lifelong chemotherapy for patients with advanced pancreatic cancer has been proposed to address chemotherapy resistance and cumulative toxicity. Poly(ADP-ribose) polymerase (PARP) inhibitors have shown efficacy in this setting, and concurrent immune checkpoint blockade could offer synergistic tumour control. The aim of this study was to test the safety and antitumour activity of maintenance with PARP inhibition combined with immune checkpoint blockade in patients with advanced pancreatic cancer who had a stable response to platinum-based chemotherapy.
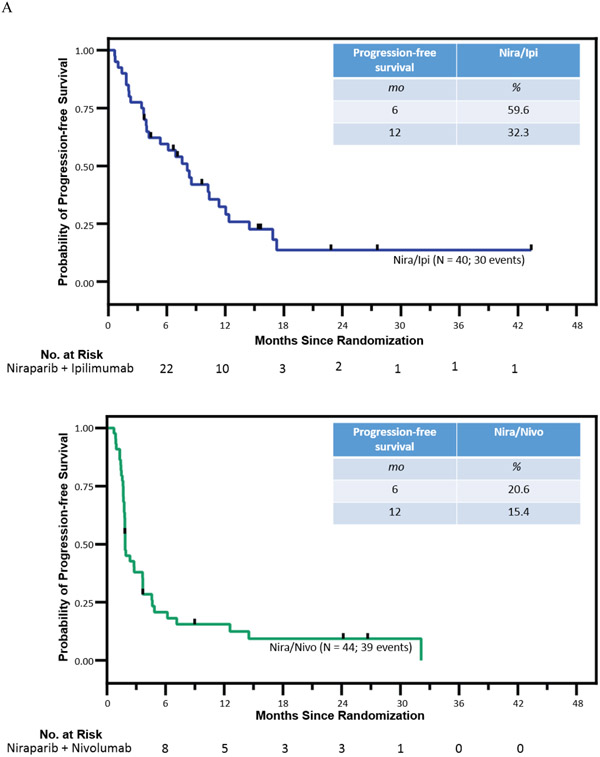
Methods: We conducted an open-label, randomised, phase 1b/2 study of niraparib plus anti-PD-1 (nivolumab) or anti-CTLA-4 (ipilimumab) therapy for patients with advanced pancreatic cancer whose cancer had not progressed after at least 16 weeks of platinum-based therapy. Patients were randomly assigned (1:1) via permuted block randomisation (block sizes 2 and 4) to niraparib 200 mg orally per day plus either nivolumab 240 mg intravenously every 2 weeks (later changed to 480 mg intravenously every 4 weeks based on manufacturer update) or ipilimumab 3 mg/kg intravenously every 4 weeks for four doses. The primary endpoints were safety and progression-free survival at 6 months. Treatment groups were not compared for activity, which was assessed in each group against a clinically meaningful progression-free survival at 6 months of 44% (null hypothesis). Superiority of a treatment regimen could be declared if 6-month progression-free survival was 60%, and inferiority if 6-month progression-free survival was 27%. All patients who received at least one dose of study treatment and had at least one post-treatment assessment of response according to Response Evaluation Criteria in Solid Tumours version 1.1 were included in the efficacy population. The safety population consisted of all patients who received at least one dose of study treatment. This study is registered with ClinicalTrials.gov, NCT03404960, and enrolment is completed and follow-up is ongoing.
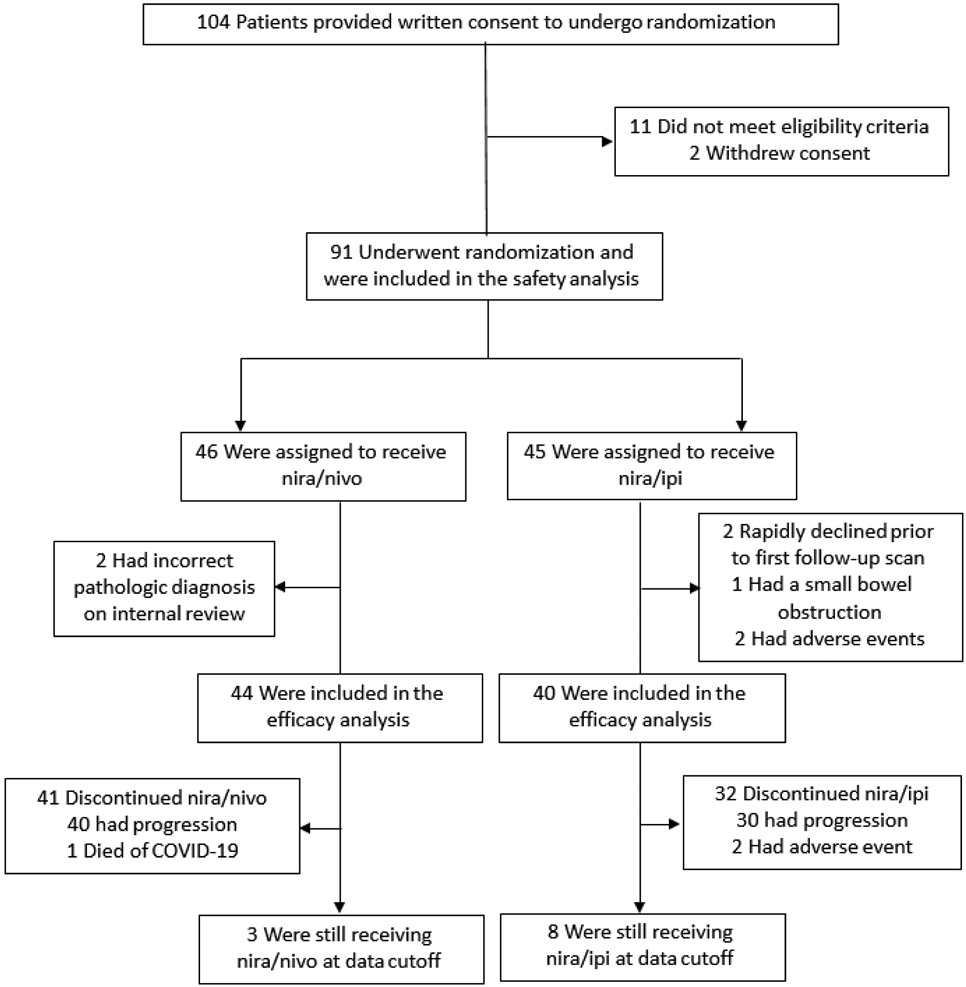
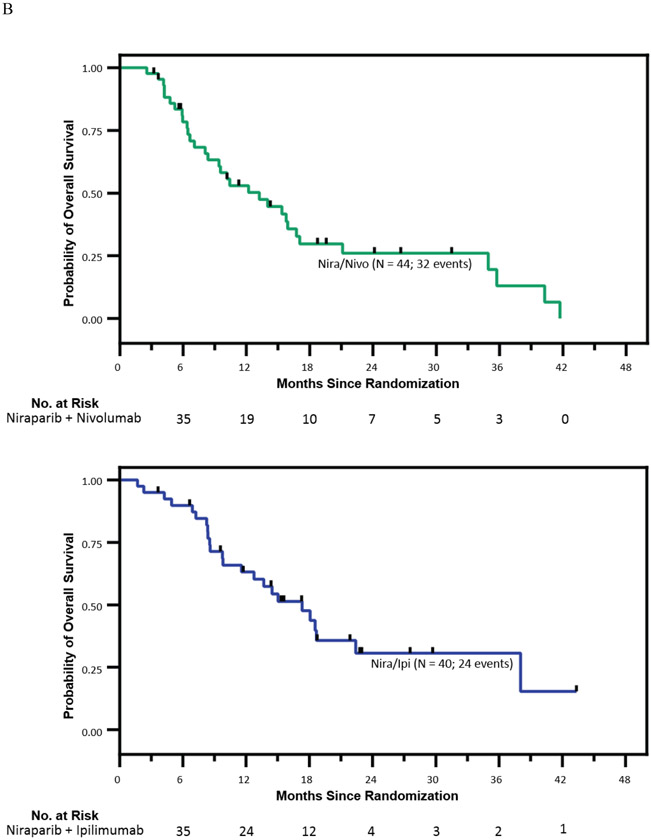
Findings: 91 patients were enrolled between Feb 7, 2018, and Oct 5, 2021 and were randomly assigned to niraparib plus nivolumab (n=46) or niraparib plus ipilimumab (n=45). Of these patients, 84 were evaluable for the progression-free survival endpoint (niraparib plus nivolumab=44; niraparib plus ipilimumab=40). Median follow-up was 23·0 months (IQR 15·0-31·5). 6-month progression-free survival was 20·6% (95% CI 8·3-32·9; p=0·0002 vs the null hypothesis of 44%) in the niraparib plus nivolumab group; and 59·6% (44·3-74·9; p=0·045) in the niraparib plus ipilimumab group. Ten (22%) of 46 patients in the niraparib plus nivolumab group and 23 (50%) of 45 patients in the niraparib plus ipilimumab group had a grade 3 or worse treatment-related adverse event. The most common grade 3 or worse adverse events in the niraparib plus nivolumab group were hypertension (in four [8%] patients), anaemia (two [4%]), and thrombocytopenia (two [4%]) whereas in the niraparib plus ipilimumab group these were fatigue (in six [14%]), anaemia (five [11%]), and hypertension (four [9%]). There were no treatment-related deaths.
Interpretation: The primary endpoint of 6-month progression-free survival was met in the niraparib plus ipilimumab maintenance group, whereas niraparib plus nivolumab yielded inferior progression-free survival. These findings highlight the potential for non-cytotoxic maintenance therapies in patients with advanced pancreatic cancer.
Funding: Bristol Myers Squibb, GlaxoSmithKline, the Basser Center Young Leadership Council, The Konner Foundation, The Pearl and Philip Basser Innovation Research Award, the Anonymous Foundation, and the US National Institutes of Health.
Copyright © 2022 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests KAR reports research support from Bristol Myers Squibb, GlaxoSmithKline, Clovis Oncology, Basser Center Young Leadership Council, Konner Foundation, Pearl and Philip Basser Innovation Research Award, and the Anonymous Foundation; honoraria from MJH Events (continuing medical education) and Dr Neil Love (continuing medical education lecture); payment for expert testimony from Aronson Rappaport Feinstein and Deutsch, LLP; support for attending a meeting from Carisma Therapeutics; and participates in the data and safety monitoring board or advisory boards for Carisma Therapeutics, AstraZeneca, and Clovis Oncology. MO reports research support from Bristol Myers Squibb, CellDex Therapeutics, Arcus, Natera, Stand Up to Cancer, and the Parker Institute for Cancer Immunotherapy; support for travel to meetings from Parker Institute for Cancer Immunotherapy and from the American Society of Clinical Oncology; and is an advisory board member of Psioxus Therapeutics. TK reports research support from Bristol Myers Squibb, Eli Lilly and Company, Syndax, Tempest Therapeutics, Taiho, H3 Biomedicine, Xencor, and Genentech; consulting fees from Ipsen, AstraZeneca, Incyte, and Exelixis; and honoraria from Pfizer. SMD reports consulting fees from AstraZeneca and GlaxoSmithKline. RHV received a research license of a research-only monoclonal antibody at Children's Hospital of Boston, MA, USA, and royalties as an inventor on a patent for cellular therapy at the University of Pennsylvania; and has leadership roles in the Association of American Cancer Institutes Board of Directors, the American Association for Cancer Research Board of Directors, National Cancer Institute Board of Scientific Advisors, the National Comprehensive Cancer Network Board of Directors, and external scientific advisory board for seven National Cancer Institute-designated cancer centres (Yale University, University of Pittsburgh Medical Center, Case Western Reserve University, Moffitt Cancer Center, University of North Carolina, New York University, and Dartmouth College). All other authors declare no competing interests.
Figures
Comment in
-
Pancreatic cancer: still a cold case?Lancet Oncol. 2022 Aug;23(8):964-965. doi: 10.1016/S1470-2045(22)00394-1. Epub 2022 Jul 7. Lancet Oncol. 2022. PMID: 35810753 No abstract available.
References
-
- Conroy T, Desseigne F, Ychou M, et al. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. The New England journal of medicine 2011; 364(19): 1817–25. - PubMed
-
- Wang-Gillam A, Hubner RA, Siveke JT, et al. NAPOLI-1 phase 3 study of liposomal irinotecan in metastatic pancreatic cancer: Final overall survival analysis and characteristics of long-term survivors. Eur J Cancer 2019; 108: 78–87. - PubMed
-
- Reiss KA, Mick R, O'Hara MH, et al. Phase II Study of Maintenance Rucaparib in Patients With Platinum-Sensitive Advanced Pancreatic Cancer and a Pathogenic Germline or Somatic Variant in BRCA1, BRCA2, or PALB2. J Clin Oncol 2021; 39(22): 2497–505. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
