

Self-reported Physical Activity and Cardiovascular Events in Adults With CKD: Findings From the CRIC (Chronic Renal Insufficiency Cohort) Study
- PMID: 35810825
- PMCID: PMC9691530
- DOI: 10.1053/j.ajkd.2022.05.007
Self-reported Physical Activity and Cardiovascular Events in Adults With CKD: Findings From the CRIC (Chronic Renal Insufficiency Cohort) Study
Abstract
Rationale & objective: In the general population, there is an association between higher levels of physical activity and lower risk for cardiovascular events and mortality, but this relationship has not been well evaluated in chronic kidney disease (CKD). We investigated the association between self-reported physical activity and outcomes in a CKD cohort.
Study design: Prospective cohort study.
Setting & participants: 3,926 participants in the Chronic Renal Insufficiency Cohort (CRIC) Study.
Exposure: Time-updated self-reported physical activity assessed by (1) quartile of moderate-to-vigorous physical activity (MVPA) and (2) meeting guideline-recommended level of physical activity (categorized as active, meeting guidelines; active, not meeting guidelines; or inactive).
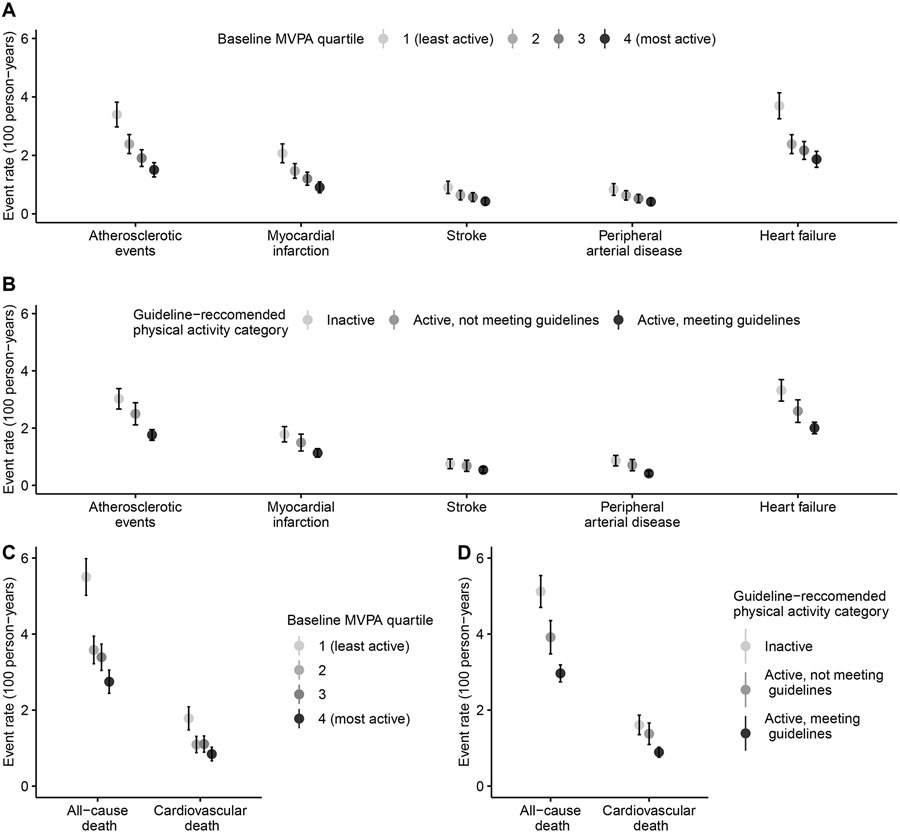
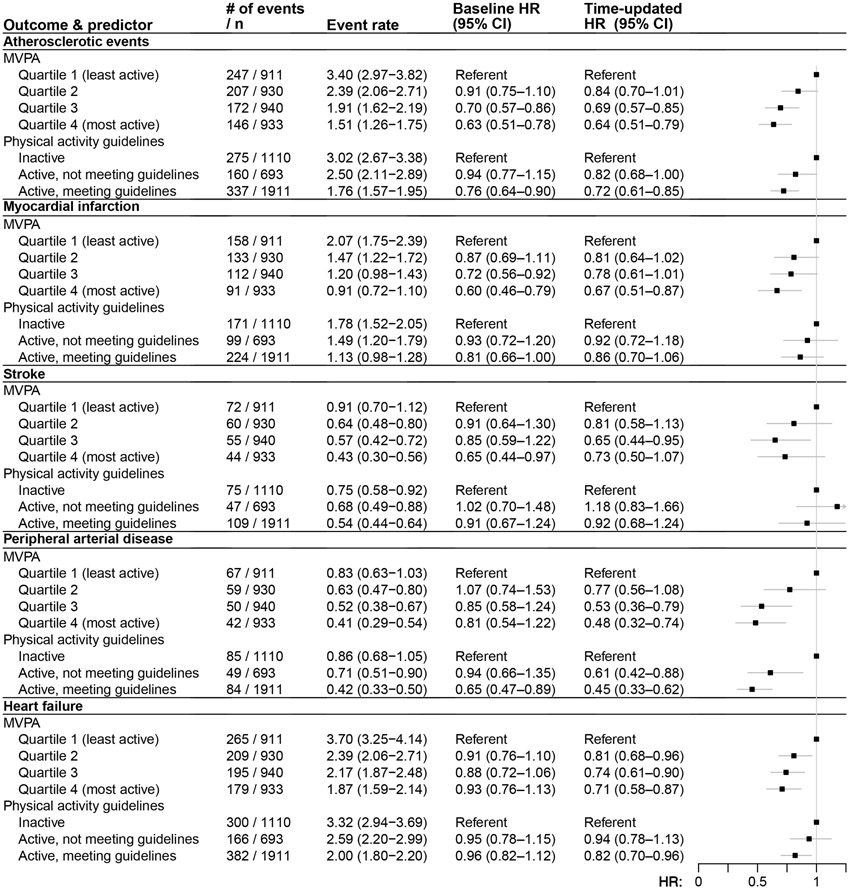
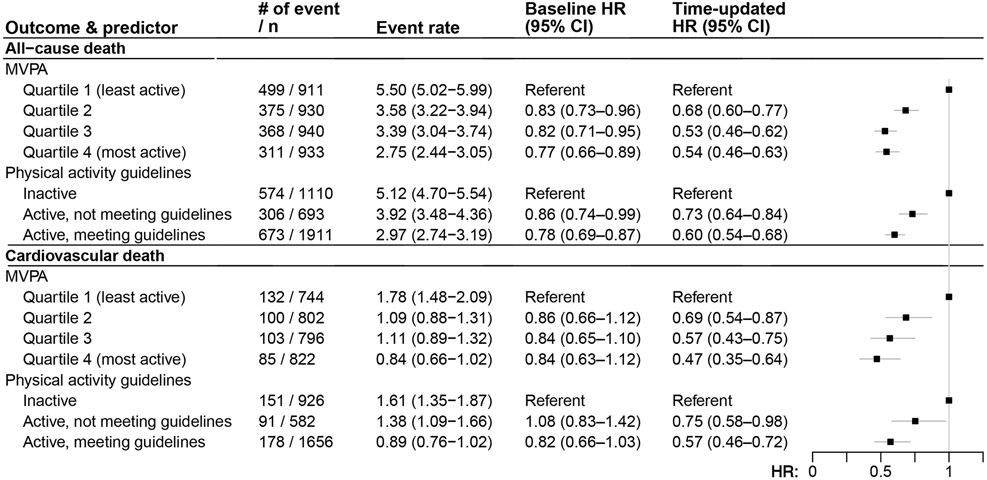
Outcome: Atherosclerotic events (myocardial infarction, stroke, or peripheral artery disease), incident heart failure, and all-cause and cardiovascular death.
Analytical approach: Cox proportional hazards regression.
Results: At baseline, compared with the lowest MVPA quartile, those in the highest quartile were more likely to be younger, male, not have prevalent cardiovascular disease, and have higher estimated glomerular filtration rate. Overall, 51% met the physical activity guidelines; of those who did not, 30% were inactive. During the median follow-up period of 13.4 years, there were 772 atherosclerotic events, 848 heart failure events, and 1,553 deaths, and 420 cardiovascular deaths. Compared with the participants in the lowest MVPA quartile, the highest quartile had a lower risk of atherosclerotic events (HR, 0.64 [95% CI, 0.51-0.79]), incident heart failure (HR, 0.71 [95% CI, 0.58-0.87]), and all-cause and cardiovascular death (HRs of 0.54 [95% CI, 0.46-0.63] and 0.47 [95% CI, 0.35-0.64], respectively). The findings were similar for analyses evaluating recommended level of physical activity.
Limitations: Self-reported physical activity may result in some degree of misclassification.
Conclusions: Higher self-reported physical activity was associated with lower risk of cardiovascular events and mortality in CKD patients, which may have important implications for clinical practice and the design of interventional studies.
Plain-language summary: In this long-term study of 3,926 adults with chronic kidney disease, we found that individuals with higher levels of physical activity were less likely to experience an atherosclerotic event (for example, a heart attack, stroke, or peripheral arterial disease), new-onset heart failure, and death as compared with those with lower levels of physical activity. The findings were similar for the analyses evaluating adherence to guideline-recommended level of physical activity (that is, for more than 150 minutes per week), and they strengthen the evidence supporting the current guideline recommendations.
Keywords: Atherosclerotic events; cardiovascular death; chronic kidney disease (CKD); exercise; health-related behavior; heart failure (HF); metabolic equivalents of task (MET); modifiable risk factor; myocardial infarction (MI); peripheral artery disease (PAD); physical exercise; stroke.
Copyright © 2022 National Kidney Foundation, Inc. Published by Elsevier Inc. All rights reserved.
Figures
Similar articles
-
Frailty and Cardiovascular Outcomes in Adults With CKD: Findings From the Chronic Renal Insufficiency Cohort (CRIC) Study.Am J Kidney Dis. 2024 Feb;83(2):208-215. doi: 10.1053/j.ajkd.2023.06.009. Epub 2023 Sep 21. Am J Kidney Dis. 2024. PMID: 37741609 Free PMC article.
-
Sex Differences in Cardiovascular Outcomes in CKD: Findings From the CRIC Study.Am J Kidney Dis. 2021 Aug;78(2):200-209.e1. doi: 10.1053/j.ajkd.2021.01.020. Epub 2021 Apr 20. Am J Kidney Dis. 2021. PMID: 33857532 Free PMC article.
-
Race/Ethnicity and Cardiovascular Outcomes in Adults With CKD: Findings From the CRIC (Chronic Renal Insufficiency Cohort) and Hispanic CRIC Studies.Am J Kidney Dis. 2016 Oct;68(4):545-553. doi: 10.1053/j.ajkd.2016.03.429. Epub 2016 May 19. Am J Kidney Dis. 2016. PMID: 27209443 Free PMC article.
-
Myeloperoxidase is Independently Associated with Incident Heart Failure in Patients with Coronary Artery Disease and Kidney Disease.Curr Probl Cardiol. 2022 Nov;47(11):101080. doi: 10.1016/j.cpcardiol.2021.101080. Epub 2021 Dec 12. Curr Probl Cardiol. 2022. PMID: 34910944 Review.
-
Physical Activity, All-Cause and Cardiovascular Mortality, and Cardiovascular Disease.Med Sci Sports Exerc. 2019 Jun;51(6):1270-1281. doi: 10.1249/MSS.0000000000001939. Med Sci Sports Exerc. 2019. PMID: 31095084 Free PMC article.
Cited by
-
Neurocirculatory regulation and adaptations to exercise in chronic kidney disease.Am J Physiol Heart Circ Physiol. 2023 Jun 1;324(6):H843-H855. doi: 10.1152/ajpheart.00115.2023. Epub 2023 Mar 31. Am J Physiol Heart Circ Physiol. 2023. PMID: 37000610 Free PMC article. Review.
-
The Role of Mitochondrial and Redox Alterations in the Skeletal Myopathy Associated with Chronic Kidney Disease.Antioxid Redox Signal. 2023 Feb;38(4-6):318-337. doi: 10.1089/ars.2022.0143. Antioxid Redox Signal. 2023. PMID: 36245209 Free PMC article. Review.
-
The effect of exercise on vascular health in chronic kidney disease: a systematic review and meta-analysis of randomized controlled trials.Am J Physiol Renal Physiol. 2023 Nov 1;325(5):F638-F655. doi: 10.1152/ajprenal.00152.2023. Epub 2023 Sep 21. Am J Physiol Renal Physiol. 2023. PMID: 37733834 Free PMC article.
-
Interventions to increase physical activity level in patients with whole spectrum chronic kidney disease: a systematic review and meta-analysis.Ren Fail. 2023;45(2):2255677. doi: 10.1080/0886022X.2023.2255677. Epub 2023 Sep 19. Ren Fail. 2023. PMID: 37724555 Free PMC article.
-
Objectively measured daily steps as an outcome in a clinical trial of chronic kidney disease: a systematic review.BMC Nephrol. 2024 Jan 3;25(1):10. doi: 10.1186/s12882-023-03412-x. BMC Nephrol. 2024. PMID: 38172696 Free PMC article.
References
-
- Kidney Disease Statistics for the United States ∣ NIDDK. National Institute of Diabetes and Digestive and Kidney Diseases. Accessed August 9, 2017. https://www.niddk.nih.gov/health-information/health-statistics/kidney-di...
-
- Chronic Kidney Disease Basics ∣ Chronic Kidney Disease Initiative ∣ CDC. Published March 9, 2021. Accessed August 6, 2021. https://www.cdc.gov/kidneydisease/basics.html
Publication types
MeSH terms
Grants and funding
- R21 DK121262/DK/NIDDK NIH HHS/United States
- UL1 TR002548/TR/NCATS NIH HHS/United States
- M01 RR013987/RR/NCRR NIH HHS/United States
- R01 DK119199/DK/NIDDK NIH HHS/United States
- UL1 TR000003/TR/NCATS NIH HHS/United States
- UL1 TR000439/TR/NCATS NIH HHS/United States
- U01 DK060990/DK/NIDDK NIH HHS/United States
- UL1 RR029879/RR/NCRR NIH HHS/United States
- U01 DK061028/DK/NIDDK NIH HHS/United States
- UL1 TR000433/TR/NCATS NIH HHS/United States
- K24 DK092290/DK/NIDDK NIH HHS/United States
- R01 DK072231/DK/NIDDK NIH HHS/United States
- U01 DK060984/DK/NIDDK NIH HHS/United States
- U01 DK061021/DK/NIDDK NIH HHS/United States
- U24 DK060990/DK/NIDDK NIH HHS/United States
- U01 DK060980/DK/NIDDK NIH HHS/United States
- T32 HL134634/HL/NHLBI NIH HHS/United States
- R01 DK124597/DK/NIDDK NIH HHS/United States
- U01 DK060963/DK/NIDDK NIH HHS/United States
- UL1 RR024131/RR/NCRR NIH HHS/United States
- R56 DK072231/DK/NIDDK NIH HHS/United States
- R01 DK118736/DK/NIDDK NIH HHS/United States
- U01 DK061022/DK/NIDDK NIH HHS/United States
- UL1 TR000424/TR/NCATS NIH HHS/United States
- M01 RR016500/RR/NCRR NIH HHS/United States
- P20 GM109036/GM/NIGMS NIH HHS/United States
- U01 DK060902/DK/NIDDK NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
