

Fatty Liver Index Independently Predicts All-Cause Mortality in Patients With Antineutrophil Cytoplasmic Antibody-Associated Vasculitis but No Substantial Liver Disease
- PMID: 35811721
- PMCID: PMC9259888
- DOI: 10.3389/fcvm.2022.848121
Fatty Liver Index Independently Predicts All-Cause Mortality in Patients With Antineutrophil Cytoplasmic Antibody-Associated Vasculitis but No Substantial Liver Disease
Abstract
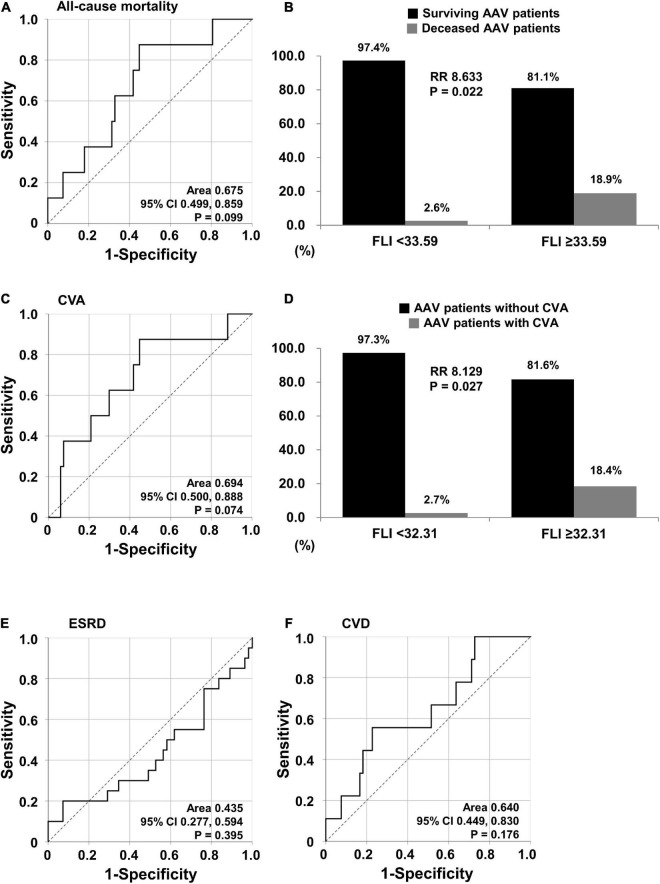
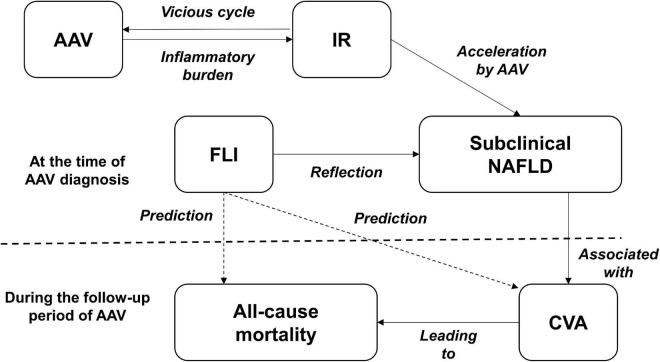
Background: This study investigated whether the fatty liver index (FLI) could predict all-cause mortality and cerebrovascular accident (CVA) during follow-up in patients with antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis (AAV) without substantial liver disease.
Methods: The medical records of 75 AAV patients with AAV were retrospectively reviewed. An equation for the FLI is as follows: FLI = (e0.953×loge(triglycerides)+0.139×BMI+0.718×loge(GGT)+0.053×waistcircumference-15.745)/(1 + e0.953×loge(triglycerides)+0.139×BMI+0.718×loge(GGT)+0.053×waistcircumference-15.745) × 100. The cut-offs of the FLI were obtained using the receiver operator characteristic (ROC) curve analysis.
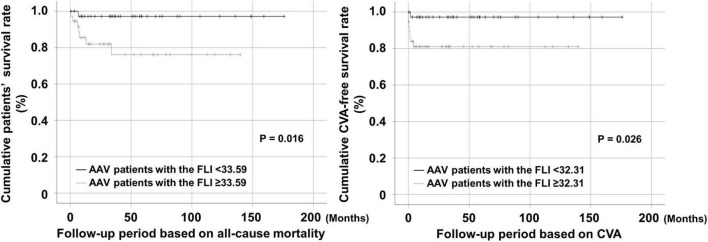
Results: The mean age at AAV diagnosis was 59.1 years and 42.7% were male. Eight patients (10.7%) died and 8 patients had CVA during follow-up. When the cut-offs of the FLI for all-cause mortality and CVA were set as the FLI ≥ 33.59 and the FLI ≥ 32.31, AAV patients with the FLI over each cut-off exhibited a higher risk for all-cause mortality or CVA than those without (RR 8.633 and 8.129), respectively. In addition, AAV patients with the FLI over each cut-off exhibited a significantly lower cumulative patients' survival rate or CVA-free survival rate than those without, respectively. In the multivariable Cox analysis, only the FLI ≥ 33.59 at AAV diagnosis was an independent predictor of all-cause mortality during follow-up in AAV patients (HR 10.448).
Conclusion: The FLI at AAV diagnosis can be a potential independent predictor of all-cause mortality and CVA during follow-up in AAV patients. We suggest that physicians measure the FLI at AAV diagnosis and pay more attention to those with a high FLI value for prevention of future mortality and CVA.
Keywords: antineutrophil cytoplasmic antibody; cerebrovascular accident; fatty liver index; mortality; vasculitis.
Copyright © 2022 Park, Pyo, Ahn, Choi, Song, Park, Huh and Lee.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Atherogenic index of plasma predicts cerebrovascular accident occurrence in antineutrophil cytoplasmic antibody-associated vasculitis.Lipids Health Dis. 2020 Aug 14;19(1):184. doi: 10.1186/s12944-020-01360-1. Lipids Health Dis. 2020. PMID: 32799861 Free PMC article.
-
Predictive potential of albumin-alkaline phosphatase ratio for cerebrovascular accident in patients with antineutrophil cytoplasmic antibody-associated vasculitis.Ann Clin Biochem. 2023 May;60(3):184-190. doi: 10.1177/00045632231154752. Epub 2023 Feb 2. Ann Clin Biochem. 2023. PMID: 36653311
-
The monocyte-to-high-density lipoprotein-cholesterol ratio at diagnosis is associated with cerebrovascular accident during follow-up in patients with antineutrophil cytoplasmic antibody-associated vasculitis.J Rheum Dis. 2024 Jul 1;31(3):151-159. doi: 10.4078/jrd.2024.0001. Epub 2024 Mar 12. J Rheum Dis. 2024. PMID: 38957360 Free PMC article.
-
Non-alcoholic fatty liver disease fibrosis score is a useful index for predicting all-cause mortality in patients with antineutrophil cytoplasmic antibody-associated vasculitis.Front Med (Lausanne). 2023 Aug 29;10:1217937. doi: 10.3389/fmed.2023.1217937. eCollection 2023. Front Med (Lausanne). 2023. PMID: 37711740 Free PMC article.
-
Antineutrophil Cytoplasmic Antibody-Associated Vasculitis in Korea: A Narrative Review.Yonsei Med J. 2019 Jan;60(1):10-21. doi: 10.3349/ymj.2019.60.1.10. Yonsei Med J. 2019. PMID: 30554486 Free PMC article. Review.
Cited by
-
Clinical Link between the BARD Score at Diagnosis and Mortality during Follow-Up in Patients with Antineutrophil Cytoplasmic Antibody-Associated Vasculitis.J Clin Med. 2023 Aug 31;12(17):5679. doi: 10.3390/jcm12175679. J Clin Med. 2023. PMID: 37685746 Free PMC article.
-
Alcoholic Liver Disease/Nonalcoholic Fatty Liver Disease Index at Diagnosis Is Associated with All-Cause Mortality during Follow-Up in Patients with Antineutrophil Cytoplasmic Antibody-Associated Vasculitis.Medicina (Kaunas). 2024 Feb 24;60(3):381. doi: 10.3390/medicina60030381. Medicina (Kaunas). 2024. PMID: 38541107 Free PMC article.
References
-
- Watts R, Lane S, Hanslik T, Hauser T, Hellmich B, Koldingsnes W, et al. Development and validation of a consensus methodology for the classification of the ANCA-associated vasculitides and polyarteritis nodosa for epidemiological studies. Ann Rheum Dis. (2007) 66:222–7. 10.1136/ard.2006.054593 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous