

Prognostic significance of diastolic dysfunction in patients with systolic dysfunction undergoing atrial fibrillation ablation
- PMID: 35812132
- PMCID: PMC9260613
- DOI: 10.1016/j.ijcha.2022.101079
Prognostic significance of diastolic dysfunction in patients with systolic dysfunction undergoing atrial fibrillation ablation
Abstract
Background: The relationship between pre-ablation left ventricular diastolic dysfunction (LVDD) and prognosis in patients with left ventricular systolic dysfunction (LVSD) undergoing atrial fibrillation (AF) ablation remains unclear.
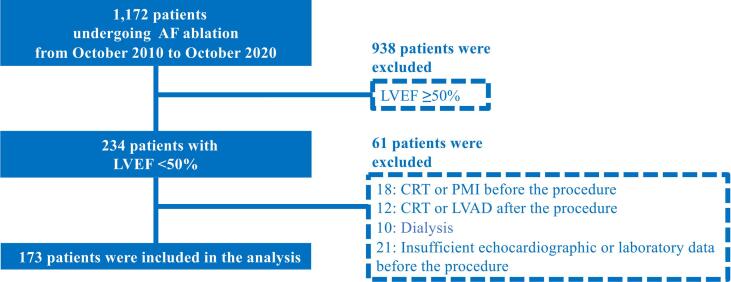
Methods: The prognosis of 173 patients with impaired left ventricular ejection fraction (<50%) who underwent AF ablation was examined. The primary outcome was a composite of all-cause mortality, heart failure (HF) hospitalization, and worsening HF symptoms requiring unplanned outpatient intensification of decongestive therapy.
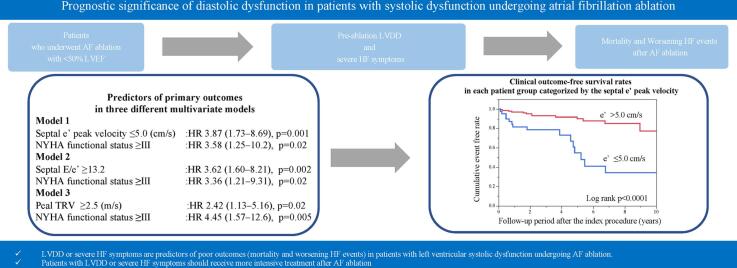
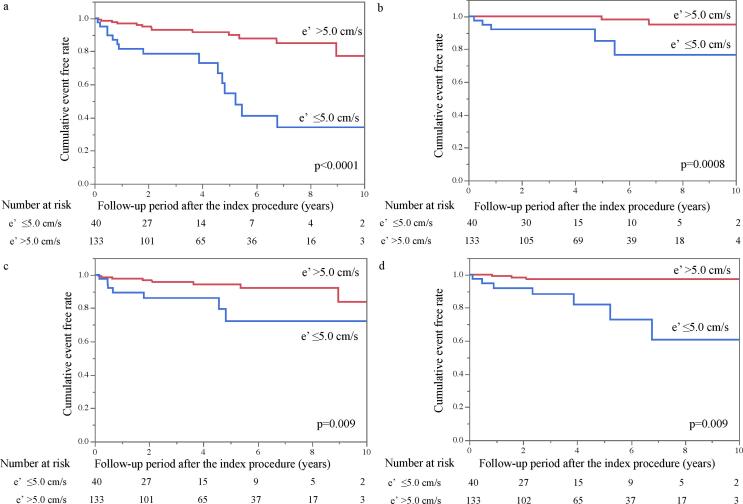
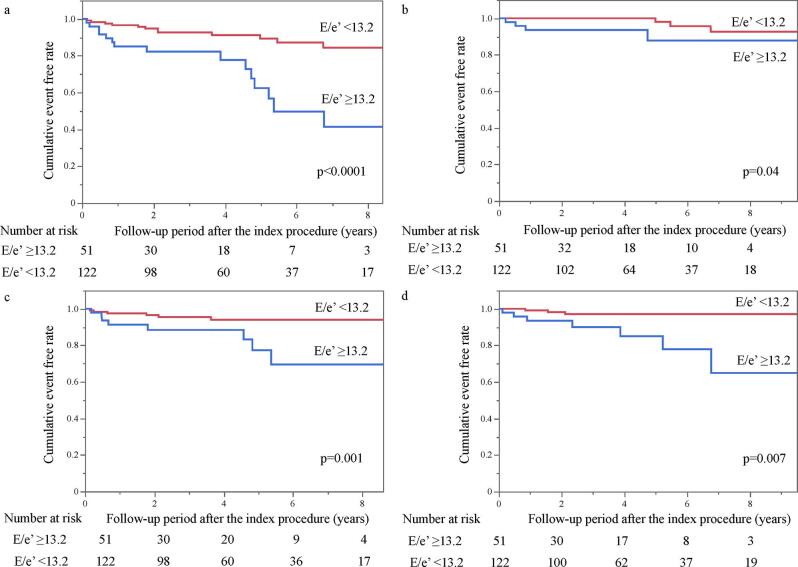
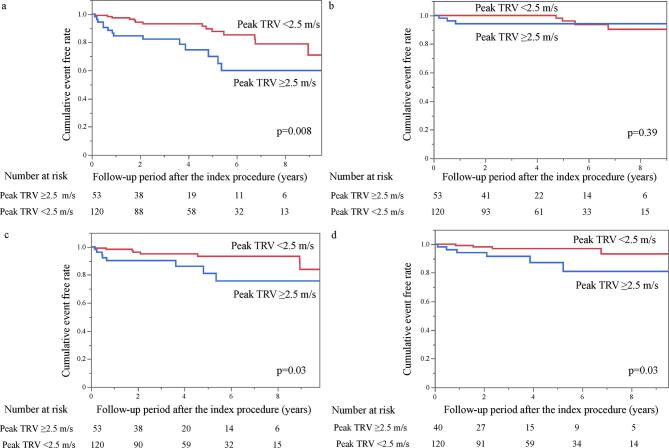
Results: During the follow-up period (median, 3.5 years), the primary outcome after AF ablation occurred in 28 patients (16%). The receiver operating characteristic curve analysis showed that early septal diastolic mitral annular velocity (e') had a larger area under the curve (0.70) than other LVDD parameters, and optimal cut-off values of LVDD, represented by e', septal E (early diastolic left ventricular filling velocity)/e', and peak tricuspid valve regurgitation velocity (TRV), were 5.0 cm/s, 13.2, and 2.5 m/s, respectively. Multivariate analysis revealed that e' ≤5.0 cm/s (standard hazard ratio [HR], 3.87; 95% confidence interval [CI], 1.73-8.69; p = 0.001), septal E/e' ≥13.2 (HR, 3.62; 95% CI, 1.60-8.21; p = 0.002), and peak TRV ≥ 2.5 m/s (HR, 2.42; 95% CI, 1.13-5.16; p = 0.02) independently predicted the outcome. Patients with New York Heart Association functional status ≥ III had a 3.3-4.5-fold higher risk of the outcome.
Conclusions: LVDD or severe HF symptoms predict poor outcomes in patients with LVSD undergoing AF ablation. Therefore, patients with LVDD or severe HF symptoms should receive more intensive treatment even after AF ablation.
Keywords: AAD, antiarrhythmic drug; AF, atrial fibrillation; AFMR, atrial functional MR; ATA, atrial tachyarrhythmia; AUC, area under the curve; Atrial fibrillation; CRT, cardiac resynchronization therapy; Catheter ablation; DT, deceleration time; Diastolic dysfunction; E, early diastolic left ventricular filling velocity; HF, heart failure; HFH, HF hospitalization; HFrEF, HF with reduced ejection fraction; Heart failure; IQR, interquartile ranges; LA, left atrial; LAVI, LA volume index; LV, left ventricular; LVAD, LV assist device; LVDD, left ventricular diastolic dysfunction; LVEF, LV ejection fraction; LVSD, left ventricular systolic dysfunction; MR, mitral regurgitation; NYHA, New York Heart Association; PAF, paroxysmal AF; PMI, pacemaker implantation; ROC, receiver operating characteristic; SD, standard deviations; SHD, structural heart disease; TRV, tricuspid valve regurgitation velocity; VFMR, ventricular functional MR; e′, early septal diastolic mitral annular velocity; rEF, reduced ejection fraction.
© 2022 The Author(s).
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
Similar articles
-
Usefulness of Preprocedural Left Ventricular End-Systolic Volume Index and Early Diastolic Mitral Annular Velocity in Predicting Improvement in Left Ventricular Ejection Fraction Following Atrial Fibrillation Ablation in Patients With Impaired Left Ventricular Systolic Function.Am J Cardiol. 2020 Mar 1;125(5):759-766. doi: 10.1016/j.amjcard.2019.11.031. Epub 2019 Dec 10. Am J Cardiol. 2020. PMID: 31889522
-
Left Ventricular Diastolic Dysfunction is Associated with Renal Dysfunction, Poor Survival and Low Health Related Quality of Life in Cirrhosis.J Clin Exp Hepatol. 2019 May-Jun;9(3):324-333. doi: 10.1016/j.jceh.2018.08.008. Epub 2018 Aug 30. J Clin Exp Hepatol. 2019. PMID: 31360025 Free PMC article.
-
The predictive value of echocardiographic parameters associated with left ventricular diastolic dysfunction on short- and long-term outcomes of catheter ablation of atrial fibrillation.Europace. 2014 Aug;16(8):1168-74. doi: 10.1093/europace/eut415. Epub 2014 Feb 25. Europace. 2014. PMID: 24569573
-
Prognostic impact of the E/e' ratio in patients with chronic severe aortic regurgitation undergoing aortic valve replacement.J Thorac Cardiovasc Surg. 2024 Jan;167(1):116-126.e1. doi: 10.1016/j.jtcvs.2022.01.036. Epub 2022 Feb 2. J Thorac Cardiovasc Surg. 2024. PMID: 35248358 Review.
-
Spironolactone to improve exercise tolerance in people with permanent atrial fibrillation and preserved ejection fraction: the IMPRESS-AF RCT.Southampton (UK): NIHR Journals Library; 2020 Jul. Southampton (UK): NIHR Journals Library; 2020 Jul. PMID: 32697452 Free Books & Documents. Review.
Cited by
-
Cardiac function and atrial conduction time in morbid obesity: Insights from an echocardiographic case-control study.Glob Cardiol Sci Pract. 2025 Feb 28;2025(1):e202513. doi: 10.21542/gcsp.2025.13. eCollection 2025 Feb 28. Glob Cardiol Sci Pract. 2025. PMID: 40390991 Free PMC article.
-
Prognostic Implications of Left Atrial Spontaneous Echo Contrast with Catheter Ablation of Nonvalvular Atrial Fibrillation Patients with Left Atrial Dilation.J Cardiovasc Dev Dis. 2022 Sep 15;9(9):306. doi: 10.3390/jcdd9090306. J Cardiovasc Dev Dis. 2022. PMID: 36135451 Free PMC article.
-
Recent highlights from the International Journal of Cardiology heart & Vasculature: Comprehensive management of atrial fibrillation.Int J Cardiol Heart Vasc. 2024 Jul 29;53:101478. doi: 10.1016/j.ijcha.2024.101478. eCollection 2024 Aug. Int J Cardiol Heart Vasc. 2024. PMID: 39175655 Free PMC article. No abstract available.
-
Recent highlights on specific aspects of oral anticoagulation in difficult clinical scenarios from the International Journal of Cardiology Heart & Vasculature.Int J Cardiol Heart Vasc. 2023 Aug 23;48:101260. doi: 10.1016/j.ijcha.2023.101260. eCollection 2023 Oct. Int J Cardiol Heart Vasc. 2023. PMID: 37663615 Free PMC article. No abstract available.
References
-
- Cha Y.M., Wokhlu A., Asirvatham S.J., et al. Success of ablation for atrial fibrillation in isolated left ventricular diastolic dysfunction: a comparison to systolic dysfunction and normal ventricular function. Circ Arrhythm Electrophysiol. 2011;4:724–732. - PubMed
-
- Hsu L.F., Jaïs P., Sanders P., et al. Catheter ablation for atrial fibrillation in congestive heart failure. N. Engl. J. Med. 2004;351:2373–2383. - PubMed
-
- Tsang T.S., Gersh B.J., Appleton C.P., et al. Left ventricular diastolic dysfunction as a predictor of the first diagnosed nonvalvular atrial fibrillation in 840 elderly men and women. J. Am. Coll. Cardiol. 2002;40:1636–1644. - PubMed
-
- Vasan R.S., Larson M.G., Levy D., et al. Doppler transmitral flow indexes and risk of atrial fibrillation (the Framingham Heart Study) Am. J. Cardiol. 2003;91:1079–1083. - PubMed
-
- Wazni O.M., Marrouche N.F., Martin D.O., et al. Radiofrequency ablation vs antiarrhythmic drugs as first-line treatment of symptomatic atrial fibrillation: a randomized trial. JAMA. 2005;293:2634–2640. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
