

Sex Differences in Clinical Characteristics, Management Strategies, and Outcomes of STEMI With COVID-19: NACMI Registry
- PMID: 35812987
- PMCID: PMC9117757
- DOI: 10.1016/j.jscai.2022.100360
Sex Differences in Clinical Characteristics, Management Strategies, and Outcomes of STEMI With COVID-19: NACMI Registry
Abstract
Background: Women with ST-segment elevation myocardial infarction (STEMI) had worse outcomes than men prior to the COVID-19 pandemic. Although concomitant COVID-19 infection increases mortality risk in STEMI patients, no studies have evaluated sex differences in this context.
Methods: The North American COVID-19 STEMI registry is a prospective, multicenter registry of hospitalized STEMI patients with COVID-19 infection. We compared sex differences in clinical characteristics, presentation, management strategies, and in-hospital mortality.
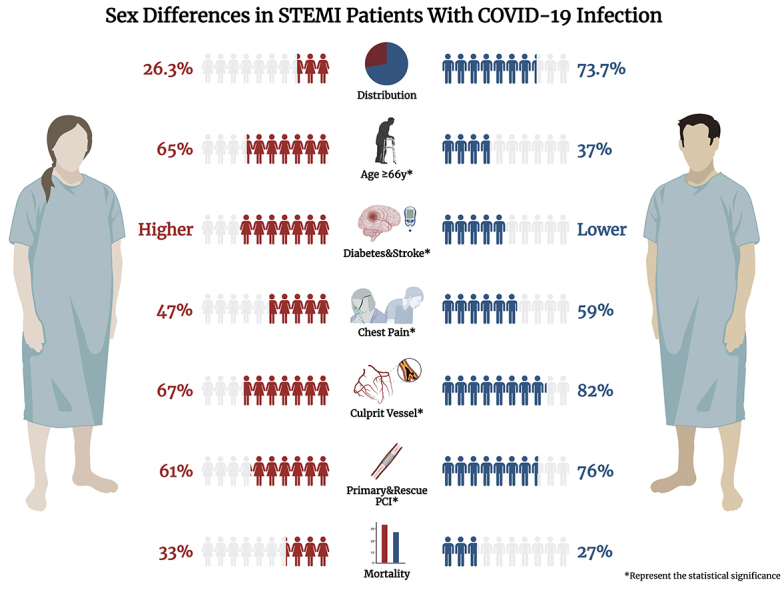
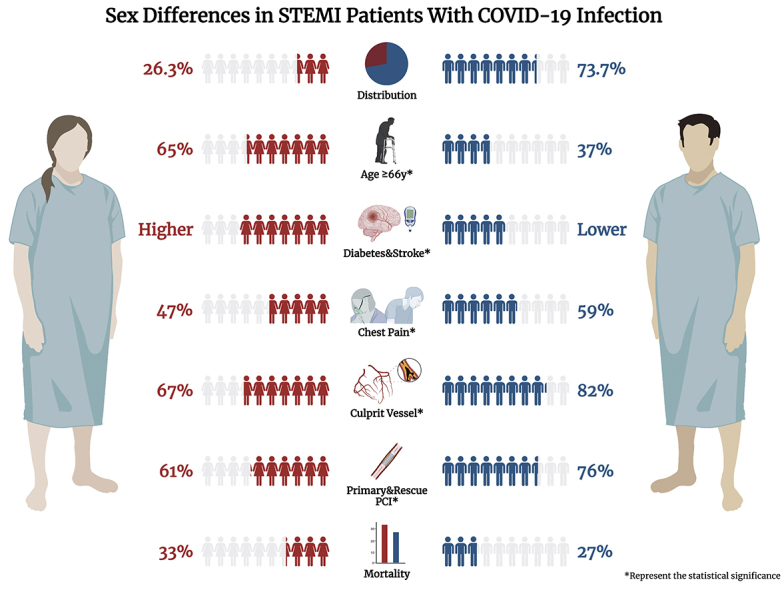
Results: Among 585 patients with STEMI and COVID-19 infection, 154 (26.3%) were women. Compared to men, women were significantly older, had a higher prevalence of diabetes and stroke/transient ischemic attack, and were more likely to be on statins on presentation. Men more frequently presented with chest pain, whereas women presented with dyspnea. Women more often had STEMI without an identified culprit lesion than men (33% vs 18%, P < .001). The use of percutaneous coronary intervention was significantly higher in men, whereas medical therapy was higher in women. In-hospital mortality was 33% for women and 27% for men (P = .22).
Conclusions: In patients presenting with STEMI in the context of COVID-19, the in-hospital mortality rate was 30% and similar for men and women. Lack of an identifiable culprit lesion was common in the setting of COVID-19 for both sexes but more likely in women (1/3 of women vs 1/5 of men). Evaluation of specific underlying etiologies is underway to better define the full impact of COVID-19 on STEMI outcomes and better understand the observed sex differences.
Keywords: COVID-19; MI, myocardial infarction; MINOCA, myocardial infarction with nonobstructive coronary artery disease; NACMI, North American COVID-19 ST-Segment Elevation Myocardial Infarction; PCI, percutaneous coronary intervention; STEMI; STEMI, ST-segment elevation myocardial infarction; TIA, transient ischemic attack; mortality; sex differences.
© 2022 The Author(s).
Conflict of interest statement
Financial support was provided by 10.13039/100004374Medtronic Inc, Abbott Cardiovascular Structural Heart Division, 10.13039/501100000106an American College of Cardiology’s Accreditation Services Foundation Committee Grant, and a Saskatchewan Health Research Foundation Grant for the NACMI registry. Dr. Quesada declared receiving grants from NIHK23HL151867. Dr. Garcia declares receiving institutional research grants from 10.13039/100006520Edwards Lifesciences, Boston Scientific, 10.13039/100004374Medtronic, and 10.13039/100011949Abbott Vascular; is a consultant for American College of Cardiology, Medtronic, and Boston Scientific; and is a proctor for Edwards Lifesciences. The remaining authors have nothing to disclose.
Figures
Comment in
-
STEMIs and a Closer Look at MINOCA During the COVID-19 Pandemic.J Soc Cardiovasc Angiogr Interv. 2022 Jul-Aug;1(4):100372. doi: 10.1016/j.jscai.2022.100372. Epub 2022 May 19. J Soc Cardiovasc Angiogr Interv. 2022. PMID: 35795878 Free PMC article. No abstract available.
References
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
