

Mirels' score for upper limb metastatic lesions: do we need a different cutoff for recommending prophylactic fixation?
- PMID: 35813136
- PMCID: PMC9264023
- DOI: 10.1016/j.jseint.2022.03.006
Mirels' score for upper limb metastatic lesions: do we need a different cutoff for recommending prophylactic fixation?
Abstract
Hypothesis: The aim of this study was to investigate the reproducibility, reliability, and accuracy of Mirels' score in upper limb bony metastatic disease and validate its use in predicting pathologic fractures.
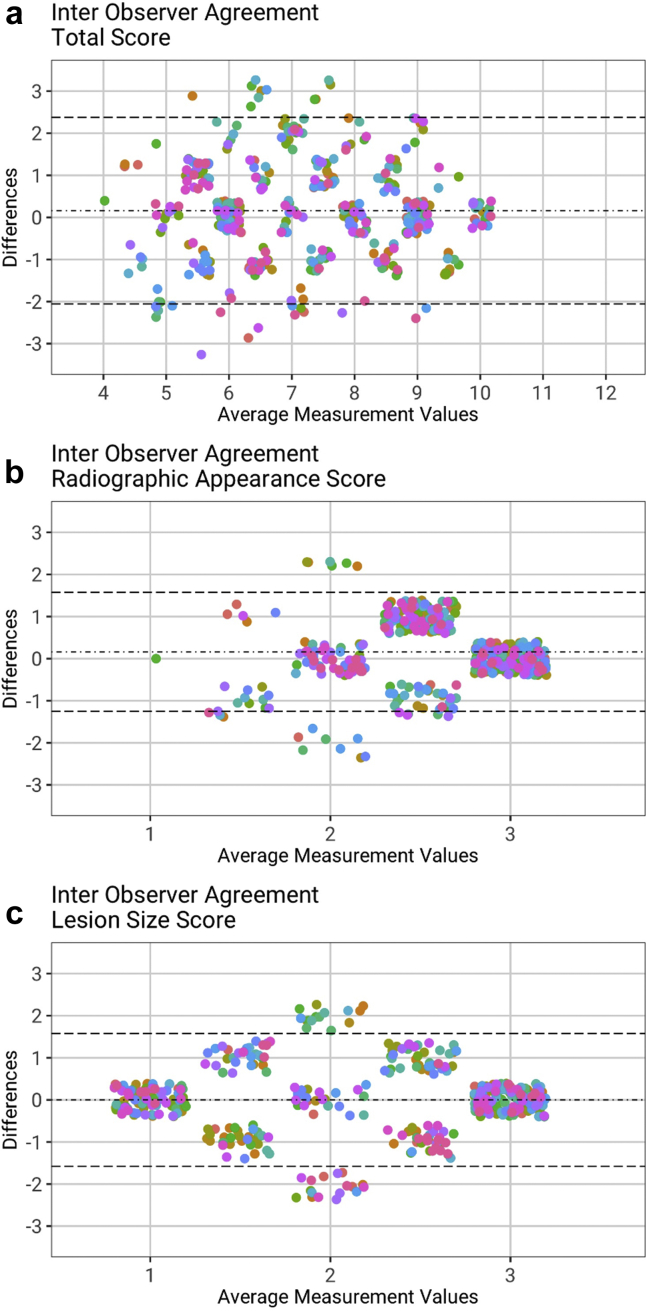
Methods: Forty-five patients with upper limb bony metastases met the inclusion criteria (62% male 28/45). The mean age was 69 years (SD 9.5), and the most common primaries were lung (29%, 13/45), followed by prostate and hematological (each 20%, 9/45). The most commonly affected bone was the humerus (76%, 35/45), followed by the ulna (6.5%, 3/45). Mirels' score was calculated in 32 patients; with plain radiographs at index presentation scored using Mirels' system by 6 raters. The radiological aspects (lesion size and appearance) were scored twice by each rater (2 weeks apart). Intraobserver and interobserver reliability were calculated using Fleiss' kappa test. Bland-Altman plots compared the variances of both individual components and the total Mirels' score.
Results: The overall fracture rate of upper limb metastatic lesions was 76% (35/46) with a mean follow-up of 3.6 years (range 11 months-6.8 years). Where time from diagnosis to fracture was known (n = 20), fractures occurred at a median 19 days (interquartile range 60-10), and 80% (16/20) occurred within 3 months of diagnosis.Mirels' score of ≥9 did not accurately predict lesions that fractured (fracture rate 11%, 5/46, for Mirels' ≥ 9 vs. 65%, 30/46, for Mirels' ≤ 8, P < .001). Sensitivity was 14%, and specificity was 73%. When Mirels' cutoff was lowered to ≥7, patients were more likely to fracture than not (48%, 22/46, vs. 28%, 13/46, P = .045); sensitivity rose to 63%, but specificity fell to 55%.Kappa values for interobserver variability were κ = 0.358 (fair, 95% confidence interval [CI] 0.288-0.429) for lesion size, κ = 0.107 (poor, 95% CI 0.02-0.193) for radiological appearance, and κ = 0.274 (fair, 95% CI 0.229-0.318) for total Mirels' score. Values for intraobserver variability were κ = 0.716 (good, 95% CI 0.432-0.999) for lesion size, κ = 0.427 (moderate, 95% CI 0.195-0.768) for radiological appearance, and κ = 0.580 (moderate, 95% CI 0.395-0.765) for total Mirels' score.
Conclusions: This study demonstrates moderate to substantial agreement between and within raters using Mirels' score on upper limb radiographs. However, Mirels' score had a poor sensitivity and specificity in predicting upper extremity fractures. Until a more valid scoring system has been developed, based on our study, we recommend a Mirels' threshold of ≥7/12 for considering prophylactic fixation of impending upper limb pathologic fractures. This contrasts with the current ≥9/12 cutoff, which is recommended for lower limb pathologic fractures.
Keywords: Metastasis; Mirels’s score; Pathological fracture; Reproducibility; Upper limb; Validity.
© 2022 Published by Elsevier Inc. on behalf of American Shoulder and Elbow Surgeons.
Figures




References
-
- British Orthopaedic Oncology Society (BOOS) Metastatic bone disease: a guide to good practice. 2015. http://www.boos.org.uk/wp-content/uploads/2016/03/BOOS-MBD-2016-BOA.pdf Available at:
-
- Cohen J. A coefficient of agreement for Nominal Scales. Educ Psychol Meas. 1960;20:37–46.
LinkOut - more resources
Full Text Sources
Miscellaneous