

Telemedicine for Stroke: Quantifying the Long-Term National Costs and Health Benefits
- PMID: 35813183
- PMCID: PMC9265143
- DOI: 10.3389/fneur.2021.804355
Telemedicine for Stroke: Quantifying the Long-Term National Costs and Health Benefits
Abstract
Objective: Few countries have established national programs to maximize access and reduce operational overheads. We aimed to use patient-level data up to 12 months to model the potential long-term costs and health benefits attributable to implementing such a program for Australia.
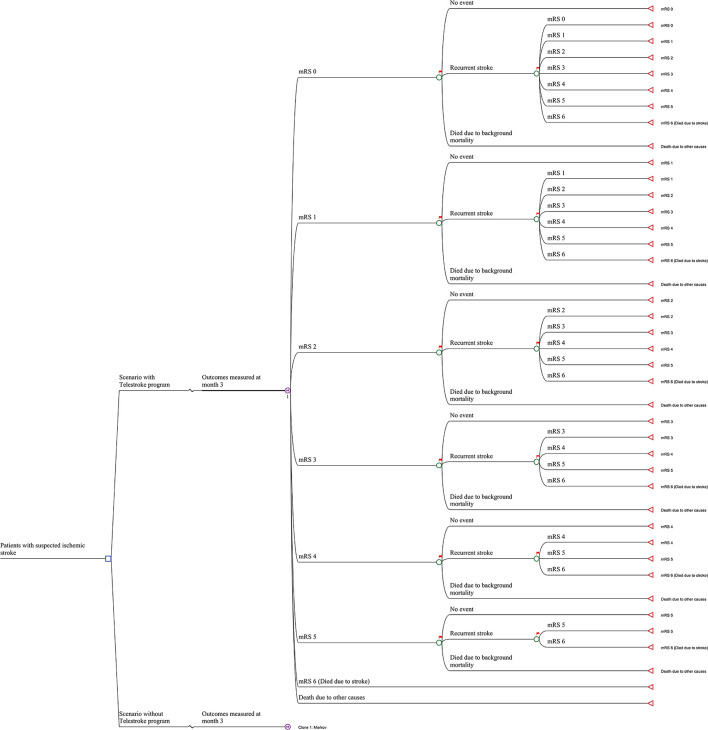
Methods: A Markov model was created for Australia with an inception population of 10,000 people with stroke presenting to non-urban or suburban hospitals without stroke medical specialists that could receive stroke telemedicine under a national program. Seven Markov states represented the seven modified Rankin Scale (mRS) scores (0 no disability to 6 dead) plus an absorbing state for all other causes of death. The literature informed inputs for the model; for the telemedicine program (including program costs and effectiveness) and patients, these were extrapolated from the Victorian Stroke Telemedicine (VST) program with the initial status of patients being their health state at day 365 as determined by their mRS score. Costs (2018 Australian dollars, healthcare, non-medical, and nursing home) and benefits were reported for both the societal and healthcare perspectives for up to a 25 years (lifetime) time horizon.
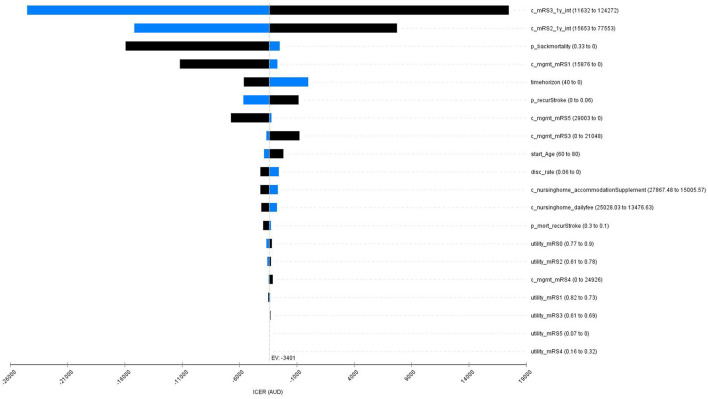
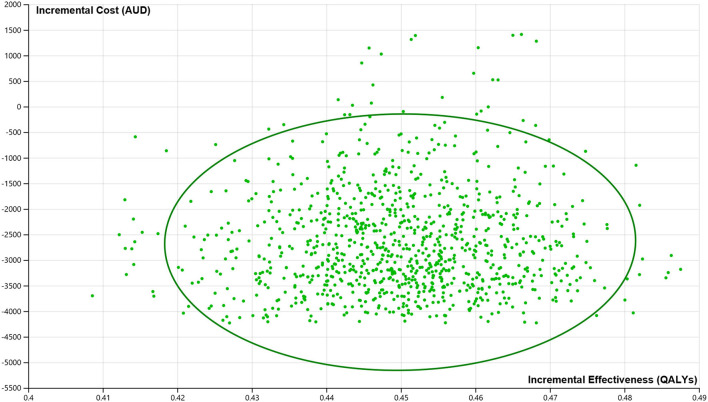
Results: We assumed 4,997 to 12,578 ischemic strokes would arrive within 4.5 h of symptom onset at regional hospitals in 2018. The average per person lifetime costs were $126,461 and $127,987 from a societal perspective or $76,680 and $75,901 from a healthcare system perspective and benefits were 4.43 quality-adjusted life years (QALYs) and 3.98 QALYs gained, respectively, for the stroke telemedicine program and practice without such program. The stroke telemedicine program was associated with a cost saving of $1,526 (from the societal perspective) or an additional $779 (from the healthcare system perspective) and an additional 0.45 QALY gained per patient over the lifetime. The incremental costs of the stroke telemedicine program ($2,959) and management poststroke ($813) were offset by cost savings from rehospitalization (-$552), nursing home care (-$2178), and non-medical resource use (-$128).
Conclusion: The findings from this long-term model provide evidence to support ongoing funding for stroke telemedicine services in Australia. Our estimates are conservative since other benefits of the service outside the use of intravenous thrombolysis were not included.
Keywords: cost-effectiveness analysis; ischemic stroke; long-term; stroke telemedicine; thrombolysis (tPA).
Copyright © 2022 Gao, Tan, Kim, Bladin, Dewey, Bagot, Cadilhac and Moodie.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Economic Evaluation Protocol and Statistical Analysis Plan for the Cost-Effectiveness of a Novel Australian Stroke Telemedicine Program; the Victorian Stroke Telemedicine (VST) program.Front Neurol. 2021 Jan 21;11:602044. doi: 10.3389/fneur.2020.602044. eCollection 2020. Front Neurol. 2021. PMID: 33584501 Free PMC article.
-
Cost-effectiveness of the Victorian Stroke Telemedicine program.Aust Health Rev. 2022 Jun;46(3):294-301. doi: 10.1071/AH21377. Aust Health Rev. 2022. PMID: 35589669
-
Cost-effectiveness of mechanical thrombectomy for acute ischemic stroke: an Australian payer perspective.J Med Econ. 2018 Aug;21(8):799-809. doi: 10.1080/13696998.2018.1474746. Epub 2018 May 30. J Med Econ. 2018. PMID: 29741126
-
Multi-gene Pharmacogenomic Testing That Includes Decision-Support Tools to Guide Medication Selection for Major Depression: A Health Technology Assessment.Ont Health Technol Assess Ser. 2021 Aug 12;21(13):1-214. eCollection 2021. Ont Health Technol Assess Ser. 2021. PMID: 34484487 Free PMC article.
-
A systematic review of cost-effectiveness analyses on endovascular thrombectomy in ischemic stroke patients.Eur Radiol. 2022 Jun;32(6):3757-3766. doi: 10.1007/s00330-022-08671-0. Epub 2022 Mar 17. Eur Radiol. 2022. PMID: 35301558
Cited by
-
Inhibition of Pyroptosis by Hydroxychloroquine as a Neuroprotective Strategy in Ischemic Stroke.eNeuro. 2024 Dec 18;12(1):ENEURO.0254-24.2024. doi: 10.1523/ENEURO.0254-24.2024. Online ahead of print. eNeuro. 2024. PMID: 39694827 Free PMC article.
-
Cost-utility tele-stroke in adults with acute ischemic stroke. A systematic review.Public Health Pract (Oxf). 2025 May 10;9:100617. doi: 10.1016/j.puhip.2025.100617. eCollection 2025 Jun. Public Health Pract (Oxf). 2025. PMID: 40487892 Free PMC article. Review.
-
The role of autologous bone in cranioplasty. A systematic review of complications and risk factors by using stored bone.Acta Neurochir (Wien). 2024 Nov 4;166(1):438. doi: 10.1007/s00701-024-06312-7. Acta Neurochir (Wien). 2024. PMID: 39495337
-
Improving patient outcomes in acute and subacute stroke using a wearable device-assisted rehabilitation system: a randomized controlled trial.J Int Med Res. 2024 Oct;52(10):3000605241281425. doi: 10.1177/03000605241281425. J Int Med Res. 2024. PMID: 39387211 Free PMC article. Clinical Trial.
References
-
- Australian Institute of Health Welfare . Stroke snapshot. (2020). Available online at: https://www.aihw.gov.au/reports/australias-health/stroke (accessed October 15, 2021).
-
- Deloitte Access Economics . Stroke in Australia – No Postcode Untouched. Melbourne. (2017).
-
- Dwyer M, Francis K, Peterson GM, Ford K, Gall S, Phan H, et al. . Regional differences in the care and outcomes of acute stroke patients in Australia: an observational study using evidence from the Australian Stroke Clinical Registry (AuSCR). BMJ Open. (2021) 11:e040418. 10.1136/bmjopen-2020-040418 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources