

Clinical outcomes and immune phenotypes associated with STK11 co-occurring mutations in non-small cell lung cancer
- PMID: 35813711
- PMCID: PMC9264081
- DOI: 10.21037/jtd-21-1377
Clinical outcomes and immune phenotypes associated with STK11 co-occurring mutations in non-small cell lung cancer
Abstract
Background: STK11 mutation in non-small cell lung cancer (NSCLC) is associated with worse survival as well as primary resistance to PD-1/PD-L1 targeting immunotherapy. We hypothesize that co-occurring mutations and tumor mutation burden (TMB) may impact response to therapy and prognosis.
Methods: Forty-one patients with STK11-mutated NSCLC seen in our Thoracic oncology clinic with available next-generation sequencing tumor data were included in the analysis. Data from the Cancer Genome Atlas (TCGA) was used for survival and immune gene expression analysis. Overall and progression-free survival (PFS) was estimated by the Kaplan-Meier method and compared using a log-rank test.
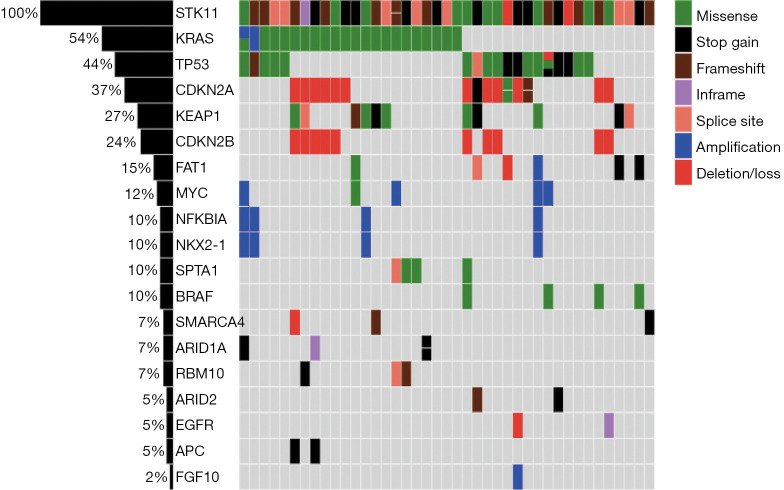
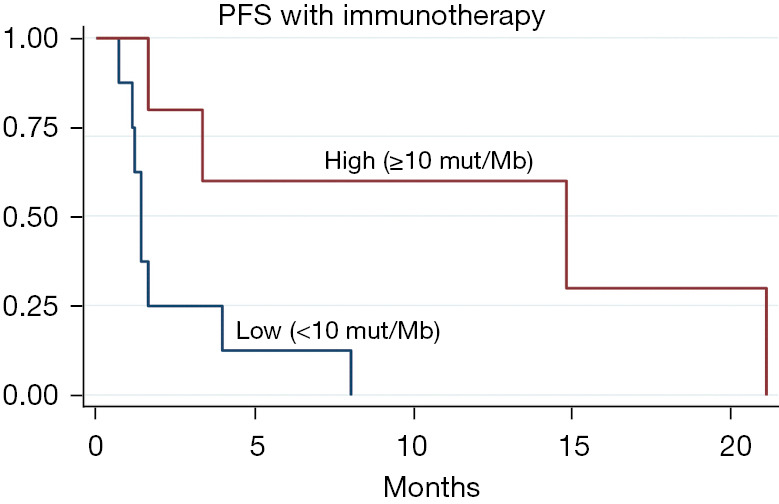
Results: In the 41 patients included, common co-occurring alterations with STK11 were KRAS (54%), TP53 (44%), CDKN2A (37%) and KEAP1 (27%). Overall 17 patients received locoregional therapy with surgery or radiation with median OS of 8.6 years and there was no significant difference in clinical outcomes with KRAS and TP53 co-occurring mutations. Response to both chemotherapy and immunotherapy was poor across all co-occurring mutations. However, TP53 co-mutation was associated with improved clinical benefit with immunotherapy. Patients with higher TMB had longer PFS with immunotherapy. In TCGA survival analysis, tumors with STK11 mutation with or without KRAS co-mutation were associated with worse survival (P<0.05) but tumors with STK11/TP53 co-mutation did not have worst survival compared to STK11 wild type tumors. Moreover, co-occurring mutations had significant effect on intratumoral immune status with both STK11 alone and STK11/KRAS co-mutated tumors showing more enrichment for wound healing immune subtype while STK11/TP53 co-mutated tumors showed more enrichment for IFN-g immune subtype.
Conclusions: Our retrospective analysis in patients with STK11-mutated NSCLC found that both TMB and co-occurring mutations may be predictors for response to immunotherapy with worse outcomes in patients with low TMB or KRAS co-mutation and improved outcomes with TP53 co-mutation. Patients with STK11-mutated NSCLC also demonstrate chemotherapy resistance but have similar outcomes with localized treatment compared to STK11 wild type tumors. Moreover, co-mutations with KRAS or TP53 significantly alter tumor immune landscape of STK11-mutated tumors and therefore response to immunotherapy.
Keywords: STK11; co-mutations; outcomes; phenotypes.
2022 Journal of Thoracic Disease. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://jtd.amegroups.com/article/view/10.21037/jtd-21-1377/coif). JM reports grants from Bristol-Myers Squibb, personal fees from Beigene, Astra Zeneca, Blueprint medicines, and Sanofi, grants from Celldex, Beyond Spring Pharma, and Biohaven, personal fees from Oncocyte, outside the submitted work. MP reports personal fees from Bayer, outside the submitted work. NC reports grants from Merck and Tempus, outside the submitted work. SKJ reports grants and personal fees from Merck, grants from Beigene, personal fees from Syntactx and IMX Medical Reviewer, outside the submitted work. The other authors have no conflicts of interest to declare.
Figures
References
-
- Skoulidis F, Byers LA, Diao L, et al. Co-occurring genomic alterations define major subsets of KRAS-mutant lung adenocarcinoma with distinct biology, immune profiles, and therapeutic vulnerabilities. Cancer Discov 2015;5:860-77. 10.1158/2159-8290.CD-14-1236 - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous