

Vessel wall magnetic resonance and arterial spin labelling imaging in the management of presumed inflammatory intracranial arterial vasculopathy
- PMID: 35813881
- PMCID: PMC9263889
- DOI: 10.1093/braincomms/fcac157
Vessel wall magnetic resonance and arterial spin labelling imaging in the management of presumed inflammatory intracranial arterial vasculopathy
Abstract
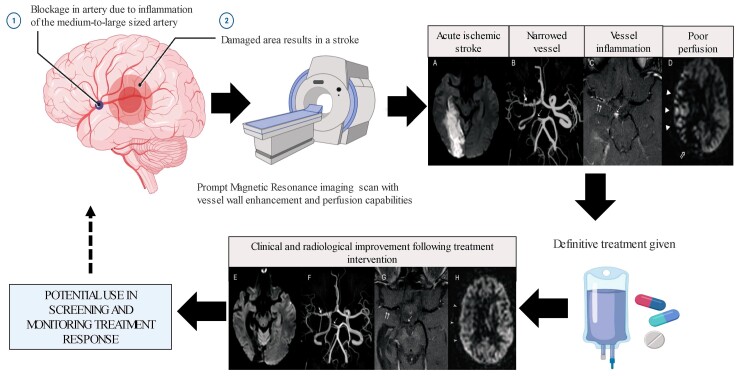
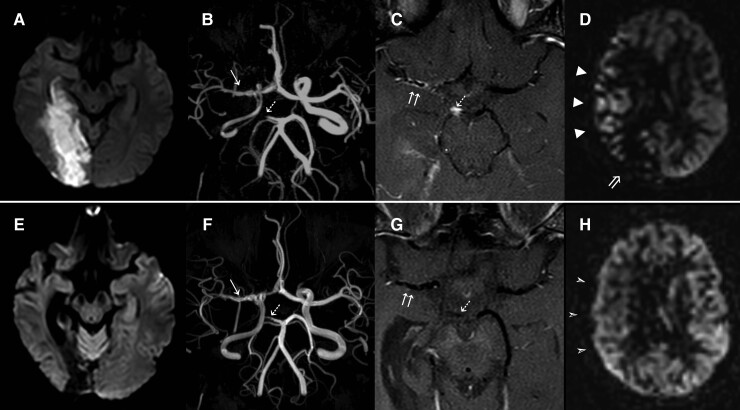
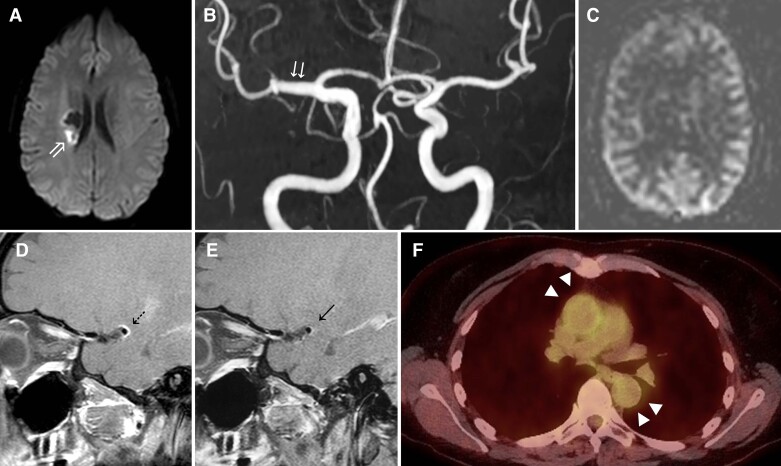
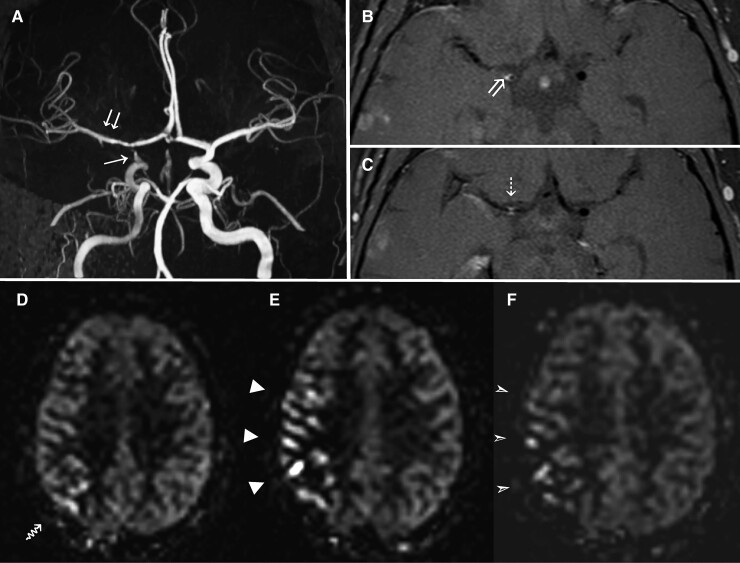
Optimal criteria for diagnosing and monitoring response to treatment for infectious and inflammatory medium-large vessel intracranial vasculitis presenting with stroke are lacking. We integrated intracranial vessel wall MRI with arterial spin labelling into our routine clinical stroke pathway to detect presumed inflammatory intracranial arterial vasculopathy, and monitor disease activity, in patients with clinical stroke syndromes. We used predefined standardized radiological criteria to define vessel wall enhancement, and all imaging findings were rated blinded to clinical details. Between 2017 and 2018, stroke or transient ischaemic attack patients were first screened in our vascular radiology meeting and followed up in a dedicated specialist stroke clinic if a diagnosis of medium-large inflammatory intracranial arterial vasculopathy was radiologically confirmed. Treatment was determined and monitored by a multi-disciplinary team. In this case series, 11 patients were managed in this period from the cohort of young stroke presenters (<55 years). The median age was 36 years (interquartile range: 33,50), of which 8 of 11 (73%) were female. Two of 11 (18%) had herpes virus infection confirmed by viral nucleic acid in the cerebrospinal fluid. We showed improvement in cerebral perfusion at 1 year using an arterial spin labelling sequence in patients taking immunosuppressive therapy for >4 weeks compared with those not receiving therapy [6 (100%) versus 2 (40%) P = 0.026]. Our findings demonstrate the potential utility of vessel wall magnetic resonance with arterial spin labelling imaging in detecting and monitoring medium-large inflammatory intracranial arterial vasculopathy activity for patients presenting with stroke symptoms, limiting the need to progress to brain biopsy. Further systematic studies in unselected populations of stroke patients are needed to confirm our findings and establish the prevalence of medium-large artery wall inflammation.
Keywords: ASL; cerebral vasculitis; neuroinflammation; stroke; vessel wall MR.
© The Author(s) 2022. Published by Oxford University Press on behalf of the Guarantors of Brain.
Figures
Similar articles
-
Vessel wall imaging: a promising enhancement in the management of inflammatory intracranial vasculopathy.Brain Commun. 2022 Sep 5;4(5):fcac226. doi: 10.1093/braincomms/fcac226. eCollection 2022. Brain Commun. 2022. PMID: 36128221 Free PMC article.
-
Intracranial Vessel Wall MRI in Cryptogenic Stroke and Intracranial Vasculitis.J Stroke Cerebrovasc Dis. 2020 May;29(5):104684. doi: 10.1016/j.jstrokecerebrovasdis.2020.104684. Epub 2020 Mar 6. J Stroke Cerebrovasc Dis. 2020. PMID: 32151477
-
Prediction of Intracranial Arterial Stenosis Progression in Patients with Moyamoya Vasculopathy: Contrast-Enhanced High-Resolution Magnetic Resonance Vessel Wall Imaging.World Neurosurg. 2018 Aug;116:e1114-e1121. doi: 10.1016/j.wneu.2018.05.181. Epub 2018 Jun 1. World Neurosurg. 2018. PMID: 29864569
-
Vessel wall MR imaging for the detection of intracranial inflammatory vasculopathies.Cardiovasc Diagn Ther. 2020 Aug;10(4):1108-1119. doi: 10.21037/cdt-20-324. Cardiovasc Diagn Ther. 2020. PMID: 32968663 Free PMC article. Review.
-
Vessel wall MR imaging of central nervous system vasculitis: a systematic review.Neuroradiology. 2022 Jan;64(1):43-58. doi: 10.1007/s00234-021-02724-9. Epub 2021 May 3. Neuroradiology. 2022. PMID: 33938989
Cited by
-
Vessel wall imaging: a promising enhancement in the management of inflammatory intracranial vasculopathy.Brain Commun. 2022 Sep 5;4(5):fcac226. doi: 10.1093/braincomms/fcac226. eCollection 2022. Brain Commun. 2022. PMID: 36128221 Free PMC article.
-
Varicella zoster vasculopathy associated with deep intracerebral haemorrhage.J Neurol. 2023 Apr;270(4):2320-2324. doi: 10.1007/s00415-022-11537-6. Epub 2022 Dec 20. J Neurol. 2023. PMID: 36538153 No abstract available.
References
-
- Rice CM, Scolding NJ. The diagnosis of primary central nervous system vasculitis. Pract Neurol. 2020;20:109–114. - PubMed
-
- Hajj-Ali RA, Singhal AB, Benseler S, Molloy E, Calabrese LH. Primary angiitis of the CNS. Lancet Neurol. 2011;10:561–572. - PubMed
-
- Salvarani C, Brown RD Jr, Christianson TJH, Huston J III, Giannini C, Hunder GG. Long-term remission, relapses and maintenance therapy in adult primary central nervous system vasculitis: A single-center 35-year experience. Autoimmun Rev. 2020;19:102497. - PubMed
-
- NICE . Stroke and transient ischaemic attack in over 16s: Diagnosis and initial management. National Institute for Health and Care Excellence; 2019. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources