

Different Anti-Vascular Endothelial Growth Factor for Patients With Diabetic Macular Edema: A Network Meta-Analysis
- PMID: 35814207
- PMCID: PMC9260109
- DOI: 10.3389/fphar.2022.876386
Different Anti-Vascular Endothelial Growth Factor for Patients With Diabetic Macular Edema: A Network Meta-Analysis
Abstract
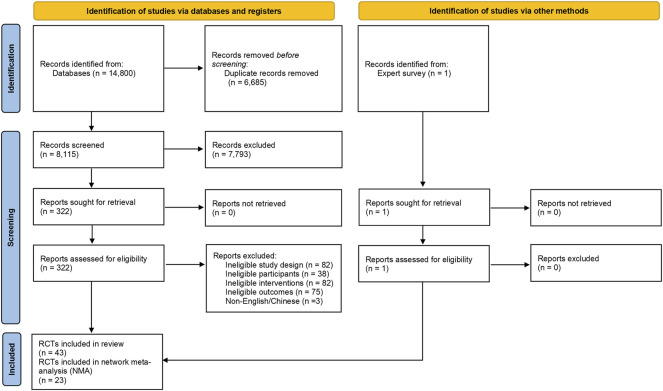
Background: Antiangiogenic therapy with anti-vascular endothelial growth factor (VEGF) is commonly used to treat diabetic macular edema (DME), which can reduce edema, improve vision, and prevent further visual loss. There is little head-to-head trial data to guide the selection of an individual VEGF inhibitor. Therefore, we aimed to investigate the efficacy and safety of anti-VEGF for patients with DME and to assess the differences between clinically relevant options by using network meta-analysis (NMA). Methods: MEDLINE, Embase, the Cochrane Library, Web of Science, Chinese Biomedical Literature Database, Wanfang, China National Knowledge Infrastructure, and VIP databases were searched for published randomized controlled trials (RCTs) from their inception to November 2020. We included RCTs of anti-VEGF drugs (intravitreal aflibercept (IVT-AFL), intravitreal ranibizumab (IVR), and intravitreal conbercept (IVC)) treating adult patients who were diagnosed with DME, regardless of stage or duration of the disease. We estimated summary odds ratios (ORs) and mean differences (MDs) with 95% credible intervals (CrIs) using a Bayesian NMA. This study's registration number is CRD42021259335. Results: We identified 43 RCTs comprising 8,234 patients. Beneficial effects were observed in patients who used IVT-AFL compared with those who used other anti-VEGF therapies at 1-year follow-up on corrected visual acuity (BCVA) improvements (all patients: versus IVR: MD 2.83, 95% CrIs 1.64, 4.01, versus IVC: MD 2.41, 95% CrIs -0.52, 5.32; patients with worse baseline visual acuity (VA): versus IVR: MD 3.39, 95% CrIs 1.89, 4.9, versus IVC: MD 3.49, 95% CrIs 0.49, 6.44) and the proportion of patients with a gain of at least 15 Early Treatment Diabetic Retinopathy Study (ETDRS) letters (all patients: versus IVR: OR 1.55, 95% CrIs 1.11, 2.17, versus IVC: OR 2.78, 95% CrIs 1.23, 6.04; patients with worse baseline VA: versus IVR: OR 2.05, 95% CrIs 1.18, 3.58, versus IVC: OR 2.85, 95% CrIs 1.24, 6.41). The effect of improvement in BCVA was identified for IVT-AFL compared to intravitreal bevacizumab. Based on the surface under the cumulative ranking curve (SUCRA), IVT-AFL had the highest probability of being the most effective option (99.9% and 99.5% in terms of the two primary outcomes, respectively). At the 2-year follow-up, numerical differences were identified favoring IVT-AFL; however, they did not reach statistical significance when comparing IVT-AFL to IVR. In the analysis of adverse events, IVT-AFL showed a lower risk of incidence of ocular adverse events compared to other anti-VEGF therapies at 1-year follow-up (versus IVR: OR 0.45, 95% CrIs 0.28, 0.7; versus IVC: OR 0.36, 95% CrIs 0.21, 0.63). Conclusion: IVT-AFL resulted in greater beneficial effects on BCVA and a higher proportion of patients with a gain of at least 15 ETDRS letters compared to IVR or IVC one year after treatment (especially in DME patients with worse baseline VA). In addition, fewer ocular adverse events occurred in the IVT-AFL group compared to the IVR or IVC groups. After two years, there was insufficient evidence to identify which anti-VEGF has superior efficacy or safety. Clinical Trial Registration: https://www.crd.york.ac.uk/prospero/, PROSPERO; https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42021259335, CRD42021259335.
Keywords: aflibercept; conbercept; diabetic macular edema; network meta-analysis; ranibizumab.
Copyright © 2022 Wang, He, Qi, Liu and Wu.
Conflict of interest statement
FQ was employed by the company Systematic Review Solutions Ltd. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Conbercept for Treatment of Neovascular Age-Related Macular Degeneration and Visual Impairment due to Diabetic Macular Edema or Pathologic Myopia Choroidal Neovascularization: A Systematic Review and Meta-Analysis.Front Pharmacol. 2021 Oct 12;12:696201. doi: 10.3389/fphar.2021.696201. eCollection 2021. Front Pharmacol. 2021. PMID: 34712132 Free PMC article. Review.
-
Anti-vascular endothelial growth factor for macular oedema secondary to branch retinal vein occlusion.Cochrane Database Syst Rev. 2020 Jul 7;7(7):CD009510. doi: 10.1002/14651858.CD009510.pub3. Cochrane Database Syst Rev. 2020. PMID: 32633861 Free PMC article.
-
Comparison of conbercept and ranibizumab for the treatment efficacy of diabetic macular edema: a Meta-analysis and systematic review.Int J Ophthalmol. 2019 Sep 18;12(9):1479-1486. doi: 10.18240/ijo.2019.09.17. eCollection 2019. Int J Ophthalmol. 2019. PMID: 31544046 Free PMC article.
-
Real-world outcomes following 12 months of intravitreal aflibercept monotherapy in patients with diabetic macular edema in France: results from the APOLLON study.Graefes Arch Clin Exp Ophthalmol. 2020 Mar;258(3):521-528. doi: 10.1007/s00417-019-04592-9. Epub 2020 Jan 2. Graefes Arch Clin Exp Ophthalmol. 2020. PMID: 31894377
-
Intravitreal Aflibercept Treatment Strategies in Routine Clinical Practice of Neovascular Age-Related Macular Degeneration in Belgium: A Retrospective Observational Study.Ophthalmol Ther. 2020 Dec;9(4):993-1002. doi: 10.1007/s40123-020-00300-7. Epub 2020 Sep 18. Ophthalmol Ther. 2020. PMID: 32946007 Free PMC article.
Cited by
-
Comparative efficacy of anti-vascular endothelial growth factor on diabetic macular edema diagnosed with different patterns of optical coherence tomography: A network meta-analysis.PLoS One. 2024 Jun 7;19(6):e0304283. doi: 10.1371/journal.pone.0304283. eCollection 2024. PLoS One. 2024. PMID: 38848379 Free PMC article.
-
Retinal vein changes in patients with high-risk proliferative diabetic retinopathy treated with conbercept and panretinal photocoagulation co-therapy: a cohort study.Front Endocrinol (Lausanne). 2023 Aug 25;14:1218442. doi: 10.3389/fendo.2023.1218442. eCollection 2023. Front Endocrinol (Lausanne). 2023. PMID: 37693359 Free PMC article.
-
Comparing the efficacy of glucocorticoids and anti-VEGF in treating diabetic macular edema: systematic review and comprehensive analysis.Front Endocrinol (Lausanne). 2024 Mar 22;15:1342530. doi: 10.3389/fendo.2024.1342530. eCollection 2024. Front Endocrinol (Lausanne). 2024. PMID: 38586457 Free PMC article.
-
Aflibercept versus ranibizumab for diabetic macular edema: A meta-analysis.Eur J Ophthalmol. 2024 May;34(3):615-623. doi: 10.1177/11206721231178658. Epub 2023 May 24. Eur J Ophthalmol. 2024. PMID: 37226427 Free PMC article. Review.
-
Anti-vascular endothelial growth factor for diabetic macular oedema: a network meta-analysis.Cochrane Database Syst Rev. 2023 Jun 27;2023(6):CD007419. doi: 10.1002/14651858.CD007419.pub7. Cochrane Database Syst Rev. 2023. PMID: 38275741 Free PMC article.
References
-
- Comyn O., Sivaprasad S., Peto T., Neveu M. M., Holder G. E., Xing W., et al. (2014). A Randomized Trial to Assess Functional and Structural Effects of Ranibizumab versus Laser in Diabetic Macular Edema (The LUCIDATE Study). Am. J. Ophthalmol. 157 (5), 960–970. 10.1016/j.ajo.2014.02.019 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous