

Reverse Triggering: An Introduction to Diagnosis, Management, and Pharmacologic Implications
- PMID: 35814233
- PMCID: PMC9256988
- DOI: 10.3389/fphar.2022.879011
Reverse Triggering: An Introduction to Diagnosis, Management, and Pharmacologic Implications
Abstract
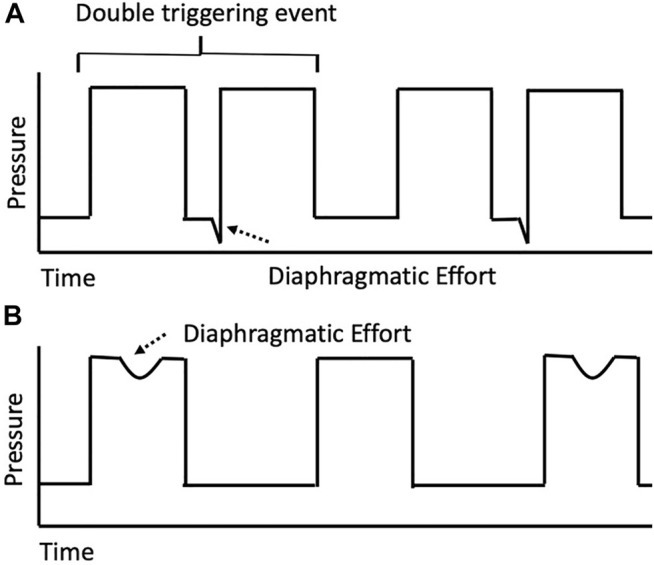
Reverse triggering is an underdiagnosed form of patient-ventilator asynchrony in which a passive ventilator-delivered breath triggers a neural response resulting in involuntary patient effort and diaphragmatic contraction. Reverse triggering may significantly impact patient outcomes, and the unique physiology underscores critical potential implications for drug-device-patient interactions. The purpose of this review is to summarize what is known of reverse triggering and its pharmacotherapeutic consequences, with a particular focus on describing reported cases, physiology, historical context, epidemiology, and management. The PubMed database was searched for publications that reported patients presenting with reverse triggering. The current body of evidence suggests that deep sedation may predispose patients to episodes of reverse triggering; as such, providers may consider decreasing sedation or modifying ventilator settings in patients exhibiting ventilator asynchrony as an initial measure. Increased clinician awareness and research focus are necessary to understand appropriate management of reverse triggering and its association with patient outcomes.
Keywords: acute respiratory distress syndrome; critical care; mechanical ventilation; respiratory failure; reverse triggering; sedation.
Copyright © 2022 Murray, Sikora, Mock, Devlin, Keats, Powell and Bice.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures


Similar articles
-
Reverse triggering during mechanical ventilation: Diagnosis and clinical implications.Med Intensiva (Engl Ed). 2023 Nov;47(11):648-657. doi: 10.1016/j.medine.2023.10.009. Epub 2023 Oct 20. Med Intensiva (Engl Ed). 2023. PMID: 37867118 Review.
-
Reverse Trigger Phenotypes in Acute Respiratory Distress Syndrome.Am J Respir Crit Care Med. 2021 Jan 1;203(1):67-77. doi: 10.1164/rccm.201907-1427OC. Am J Respir Crit Care Med. 2021. PMID: 32809842 Free PMC article.
-
Patient-ventilator asynchrony during daily interruption of sedation versus no sedation protocol.Anesth Essays Res. 2012 Jul-Dec;6(2):151-6. doi: 10.4103/0259-1162.108296. Anesth Essays Res. 2012. PMID: 25885608 Free PMC article.
-
Frequency and Risk Factors for Reverse Triggering in Pediatric Acute Respiratory Distress Syndrome during Synchronized Intermittent Mandatory Ventilation.Ann Am Thorac Soc. 2021 May;18(5):820-829. doi: 10.1513/AnnalsATS.202008-1072OC. Ann Am Thorac Soc. 2021. PMID: 33326335 Free PMC article. Clinical Trial.
-
Ventilator triggering.J Pediatr Intensive Care. 2013 Mar;2(1):11-18. doi: 10.3233/PIC-13043. Epub 2015 Jul 28. J Pediatr Intensive Care. 2013. PMID: 31214418 Free PMC article. Review.
Cited by
-
Driving pressure in mechanical ventilation: A review.World J Crit Care Med. 2024 Mar 9;13(1):88385. doi: 10.5492/wjccm.v13.i1.88385. eCollection 2024 Mar 9. World J Crit Care Med. 2024. PMID: 38633474 Free PMC article. Review.
References
-
- Acute Respiratory Distress Syndrome N., Brower R. G., Matthay M. A., Morris A., Schoenfeld D., Thompson B. T., et al. (2000). Ventilation with Lower Tidal Volumes as Compared with Traditional Tidal Volumes for Acute Lung Injury and the Acute Respiratory Distress Syndrome. N. Engl. J. Med. 342, 1301–1308. 10.1056/NEJM200005043421801 - DOI - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources