

Preoperative Prediction of the Aggressiveness of Oral Tongue Squamous Cell Carcinoma with Quantitative Parameters from Dual-Energy Computed Tomography
- PMID: 35814448
- PMCID: PMC9260668
- DOI: 10.3389/fonc.2022.904471
Preoperative Prediction of the Aggressiveness of Oral Tongue Squamous Cell Carcinoma with Quantitative Parameters from Dual-Energy Computed Tomography
Abstract
Objectives: To determine whether quantitative parameters derived from dual-energy computed tomography (DECT) were predictive of the aggressiveness of oral tongue squamous cell carcinoma (OTSCC) including the pathologic stages, histologic differentiation, lymph node status, and perineural invasion (PNI).
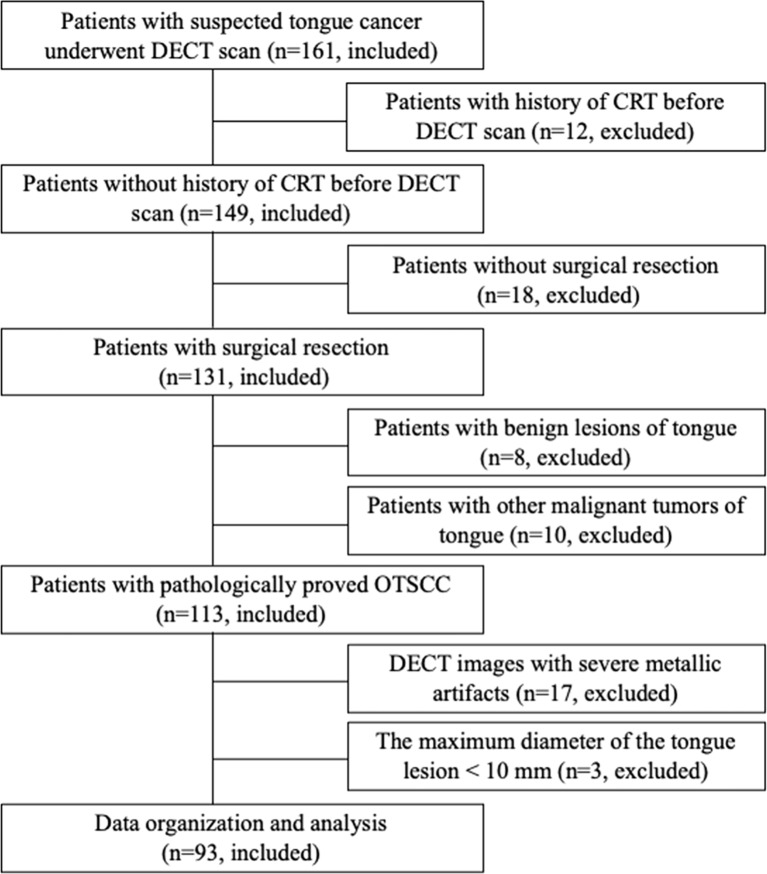
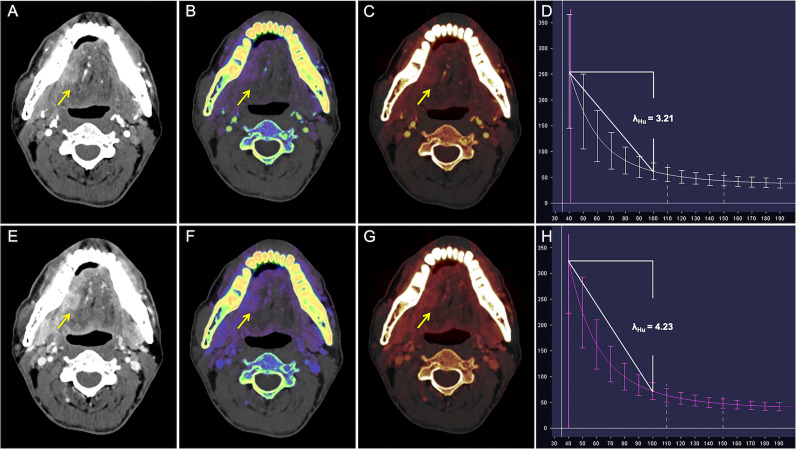
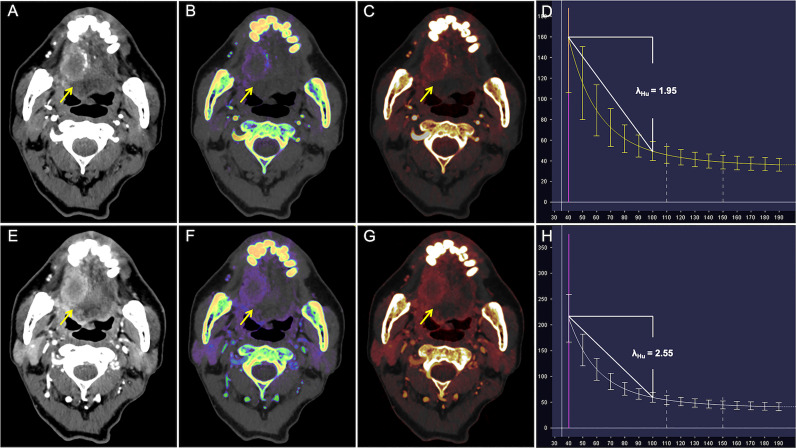
Methods: Between August 2019 and March 2021, 93 patients (mean age, 54.6 ± 13.8 years; 66 men) with pathologically diagnosed OTSCC were enrolled in this prospective study. Preoperative DECT was performed and quantitative parameters (e.g., slope of the spectral Hounsfield unit curve [λHu], normalized iodine concentration [nIC], normalized effective atomic number [nZeff], and normalized electron density [nRho]) were measured on arterial phase (AP) and venous phase (VP) DECT imaging. Quantitative parameters from DECT were compared between patients with different pathologic stages, histologic differentiation, lymph node statuses, and perineural invasion statuses. Logistic regression analysis was utilized to assess independent parameters and the diagnostic performance was analyzed by the receiver operating characteristic curves (ROC).
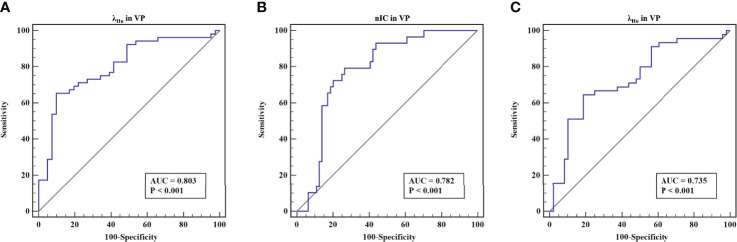
Results: λHu and nIC in AP and λHu, nZeff, and nIC in VP were significantly lower in stage III-IV lesions than in stage I-II lesions (p < 0.001 to 0.024). λHu in VP was an independent predictor of tumor stage with an odds ratio (OR) of 0.29, and area under the curve (AUC) of 0.80. λHu and nIC were higher in well-differentiated lesions than in poorly differentiated lesions (p < 0.001 to 0.021). The nIC in VP was an independent predictor of histologic differentiation with OR of 0.31, and AUC of 0.78. λHu and nIC in VP were lower in OTSCCs with lymph node metastasis than those without metastasis (p < 0.001 to 0.005). λHu in VP was the independent predictor of lymph node status with OR of 0.42, and AUC of 0.74. No significant difference was found between OTSCCs without PNI and those with PNI in terms of the quantitative DECT parameters.
Conclusion: DECT can be a complementary means for the preoperative prediction of the aggressiveness of OTSCC.
Keywords: Aggressiveness; Dual-energy CT; Oral tongue squamous cell carcinoma; histologic differentiation; lymph node status; pathologic stages.
Copyright © 2022 Yang, Hu, Zhang, Li, Yang, Shi, Lu, Jiang, Yang, Wang, Duan and Shen.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Evaluation of Quantitative Dual-Energy Computed Tomography Parameters for Differentiation of Parotid Gland Tumors.Acad Radiol. 2024 May;31(5):2027-2038. doi: 10.1016/j.acra.2023.08.024. Epub 2023 Sep 18. Acad Radiol. 2024. PMID: 37730491
-
Dual-energy CT quantitative parameters for prediction of prognosis in patients with resectable rectal cancer.Eur Radiol. 2025 Aug;35(8):4945-4956. doi: 10.1007/s00330-025-11398-3. Epub 2025 Feb 8. Eur Radiol. 2025. PMID: 39921716
-
Quantitative parameters of dual-layer spectral detector computed tomography for evaluating differentiation grade and lymphovascular and perineural invasion in colorectal adenocarcinoma.Eur J Radiol. 2024 Sep;178:111594. doi: 10.1016/j.ejrad.2024.111594. Epub 2024 Jun 28. Eur J Radiol. 2024. PMID: 38986232
-
Using quantitative parameters derived from pretreatment dual-energy computed tomography to predict histopathologic features in head and neck squamous cell carcinoma.Quant Imaging Med Surg. 2022 Feb;12(2):1243-1256. doi: 10.21037/qims-21-650. Quant Imaging Med Surg. 2022. PMID: 35111620 Free PMC article.
-
[Comparative imaging study of mediastinal lymph node from pre-surgery dual energy CT versus post-surgeron verifications in non-small cell lung cancer patients].Beijing Da Xue Xue Bao Yi Xue Ban. 2020 Aug 18;52(4):730-737. doi: 10.19723/j.issn.1671-167X.2020.04.026. Beijing Da Xue Xue Bao Yi Xue Ban. 2020. PMID: 32773811 Free PMC article. Chinese.
Cited by
-
Value of dual-layer spectral detector computed tomography in the diagnosis of benign/malignant solid solitary pulmonary nodules and establishment of a prediction model.Front Oncol. 2023 May 5;13:1147479. doi: 10.3389/fonc.2023.1147479. eCollection 2023. Front Oncol. 2023. PMID: 37213284 Free PMC article.
-
Head and Neck Squamous Cell Carcinoma: Insights from Dual-Energy Computed Tomography (DECT).Tomography. 2024 Nov 11;10(11):1780-1797. doi: 10.3390/tomography10110131. Tomography. 2024. PMID: 39590940 Free PMC article. Review.
-
The preoperative prediction of lymph node metastasis of resectable pancreatic ductal adenocarcinoma using dual-layer spectral computed tomography.Eur Radiol. 2025 May;35(5):2692-2701. doi: 10.1007/s00330-024-11143-2. Epub 2024 Oct 24. Eur Radiol. 2025. PMID: 39448418
-
Dual-Energy Computed Tomography Parameters Combined With Inflammatory Indicators Predict Cervical Lymph Node Metastasis in Papillary Thyroid Cancer.Cancer Control. 2024 Jan-Dec;31:10732748241262177. doi: 10.1177/10732748241262177. Cancer Control. 2024. PMID: 38881040 Free PMC article.
-
Dual-energy computed tomography for predicting cervical lymph node metastasis in laryngeal squamous cell carcinoma.Heliyon. 2024 Jul 31;10(16):e35528. doi: 10.1016/j.heliyon.2024.e35528. eCollection 2024 Aug 30. Heliyon. 2024. PMID: 39229502 Free PMC article.
References
-
- Institute NC Cancer Stat Facts: Oral Cavity and Pharynx Cancer. Available at: https://seer.cancer.gov/statfacts/html/oralcav.html. Accessed 25 Oct 2020.
LinkOut - more resources
Full Text Sources