

Surgical Risk Assessment in Patients with Chronic Liver Diseases
- PMID: 35814505
- PMCID: PMC9257927
- DOI: 10.1016/j.jceh.2022.03.004
Surgical Risk Assessment in Patients with Chronic Liver Diseases
Abstract
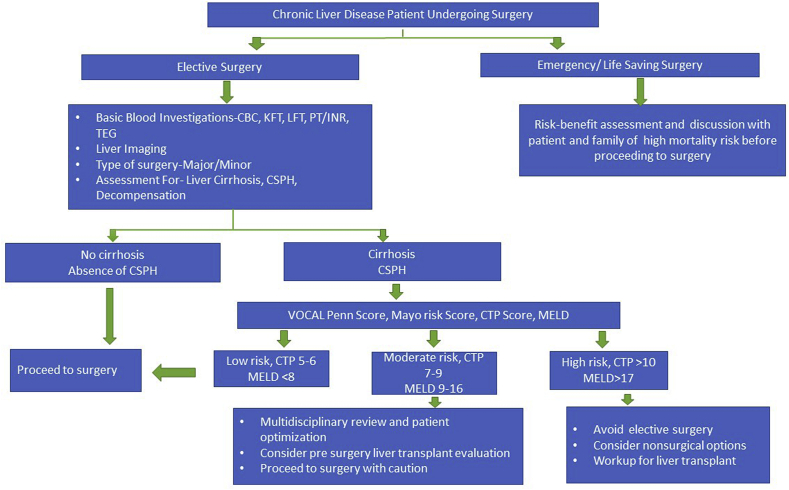
Chronic liver diseases (CLD) is one of the leading causes of morbidity and mortality. The overall life span of patients with CLD has increased and so is the number of surgical procedures these patients undergo. Pathophysiological and hemodynamic changes in cirrhosis make these patients more susceptible to hypotension and hypoxia during surgery. They also have a high risk of drug induced liver injury, renal dysfunction and post-operative liver decompensation. Patients with CLD planned for elective or semi-elective surgery should undergo detailed preoperative risk assessment. Patients should be evaluated for the presence of clinically significant portal hypertension and cirrhosis. In the absence of both cirrhosis and clinically significant portal hypertension, patients with CLD can undergo surgery with minimal or low risk. Various risk assessment tools available for patients with advanced CLD are-CTP score, MELD Score, Mayo risk score, VOCAL-Penn score. A Child class C and/or Mayo risk score >15 in general is associated with high risk of post-operative mortality and elective surgery should be deferred in these patients. In patients with Child class, A and MELD 10-15 surgery is permissible with caution (except liver resection and cardiac surgery) while in Child A and MELD <10 surgery is well tolerated. VOCAL-Penn score is a new promising tool and can be the better alternative of CTP, MELD, and Mayo risk score models but more prospective studies with large patients' population are warranted. Certain surgeries like Hepatic resection, intraabdominal, and cardiothoracic have higher risk than abdominal wall hernia repair and orthopedic surgery. Laparoscopic approaches have better outcomes and less risk of liver failure than open surgery. Minimally invasive alternatives like colonic stent placement in case of obstruction can be considered in high-risk cases. Perioperative optimization and management of ascites, HE, bleeding, liver decompensation, and nutrition should be done with multidisciplinary approach. Patients with cirrhosis undergoing high risk elective surgery can develop liver failure in post-operative period and should be evaluated and counseled for liver transplantation if not contraindicated.
Keywords: ASA, American Society of Anaesthesiologists; CLD, Chronic liver disease; CTP, Child-Turcotte-Pugh; Cirrhosis; HCC, Hepatocellular carcinoma; HVPG, hepatic venous pressure gradient; MELD, Model for end stage liver disease; NASH, Non-alcoholic steatohepatitis; ROTEM, rotational thromboelastometry; Surgery in cirrhosis; Surgical risk assessment; TEG, Thromboelastography; VOCAL-Penn score, Veterans Outcomes and Costs Associated with Liver Disease-Penn score.
© 2022 Indian National Association for Study of the Liver. Published by Elsevier B.V. All rights reserved.
Figures
Similar articles
-
Surgery in a patient with liver disease.J Clin Exp Hepatol. 2012 Sep;2(3):238-46. doi: 10.1016/j.jceh.2012.05.003. Epub 2012 Sep 21. J Clin Exp Hepatol. 2012. PMID: 25755440 Free PMC article. Review.
-
The prognostic role of hepatic venous pressure gradient in cirrhotic patients undergoing elective extrahepatic surgery.J Hepatol. 2019 Nov;71(5):942-950. doi: 10.1016/j.jhep.2019.07.007. Epub 2019 Jul 19. J Hepatol. 2019. PMID: 31330170
-
Risk Prediction Models for Post-Operative Mortality in Patients With Cirrhosis.Hepatology. 2021 Jan;73(1):204-218. doi: 10.1002/hep.31558. Epub 2020 Dec 10. Hepatology. 2021. PMID: 32939786 Free PMC article.
-
Overview of Complications in Cirrhosis.J Clin Exp Hepatol. 2022 Jul-Aug;12(4):1150-1174. doi: 10.1016/j.jceh.2022.04.021. Epub 2022 May 14. J Clin Exp Hepatol. 2022. PMID: 35814522 Free PMC article. Review.
-
Liver resection for hepatocellular carcinoma in patients with clinically significant portal hypertension.JHEP Rep. 2020 Oct 8;3(1):100190. doi: 10.1016/j.jhepr.2020.100190. eCollection 2021 Feb. JHEP Rep. 2020. PMID: 33294830 Free PMC article.
Cited by
-
Ultrasound-Guided Rectus Sheath Block With Monitored Anesthesia Care for Necrotic Umbilical Hernia Repair in a Patient With Severe Liver Failure and Refractory Ascites: A Case Report.Cureus. 2025 Mar 11;17(3):e80433. doi: 10.7759/cureus.80433. eCollection 2025 Mar. Cureus. 2025. PMID: 40083587 Free PMC article.
-
New Indications for TIPSs: What Do We Know So Far?J Clin Exp Hepatol. 2023 Sep-Oct;13(5):794-803. doi: 10.1016/j.jceh.2023.01.017. Epub 2023 Feb 10. J Clin Exp Hepatol. 2023. PMID: 37693277 Free PMC article. Review.
-
Devices for minimally invasive liver parenchyma transection: the SICE (Italian Society of Endoscopic Surgery) Italian and International survey.Surg Endosc. 2025 Aug;39(8):4822-4838. doi: 10.1007/s00464-025-11769-3. Epub 2025 Jun 16. Surg Endosc. 2025. PMID: 40523976 Free PMC article.
-
Not just a clearance: Surgical risk in patients with cirrhosis.Clin Liver Dis (Hoboken). 2024 Mar 7;23(1):e0109. doi: 10.1097/CLD.0000000000000109. eCollection 2024 Jan-Jun. Clin Liver Dis (Hoboken). 2024. PMID: 38455234 Free PMC article. Review. No abstract available.
-
Increased preoperative aspartate aminotransferase-to-platelet ratio index predicts complications following total shoulder arthroplasty.JSES Int. 2023 Jul 3;7(5):855-860. doi: 10.1016/j.jseint.2023.06.006. eCollection 2023 Sep. JSES Int. 2023. PMID: 37719816 Free PMC article.
References
-
- Reverter E., Cirera I., Albillos A., et al. The prognostic role of hepatic venous pressure gradient in cirrhotic patients undergoing elective extrahepatic surgery. J Hepatol. 2019 Nov;71:942–950. - PubMed
-
- Sheen I.-S., Liaw Y.-F. The prevalence and incidence of cholecystolithiasis in patients with chronic liver diseases: a prospective study. Hepatology. 1989;9:538–540. - PubMed
-
- Sørensen H.T., Friis S., Olsen J.H., et al. Risk of liver and other types of cancer in patients with cirrhosis: a nationwide cohort study in Denmark. Hepatology. 1998;28:921–925. - PubMed
-
- Northup P.G., Friedman L.S., Kamath P.S. AGA clinical practice update on surgical risk assessment and perioperative management in cirrhosis: expert review. Clin Gastroenterol Hepatol. 2019 Mar;17:595–606. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
