

Postreperfusion Liver Biopsy as Predictor of Early Graft Dysfunction and Survival After Orthotopic Liver Transplantation
- PMID: 35814514
- PMCID: PMC9257905
- DOI: 10.1016/j.jceh.2021.12.015
Postreperfusion Liver Biopsy as Predictor of Early Graft Dysfunction and Survival After Orthotopic Liver Transplantation
Abstract
Background: Postreperfusion liver biopsy (PRB) can assess the degree of ischemia/reperfusion injury (IRI) after orthotopic liver transplantation (OLT). The influence of IRI on graft outcomes and overall survival is controversial.
Aim: To determine the correlation between the severity of IRI in PRB and overall graft and patient survival and, secondarily, to identify factors on PRB that predict poor graft outcomes.
Methods: This is a retrospective analysis of all patients who underwent OLT using donation after brain death (DBD) with PRB. The severity of IRI in PRB was graded. Predictors of IRI were assessed using univariate and multivariate analysis and the Kaplan-Meier with log rank test for the graft and overall survival, respectively.
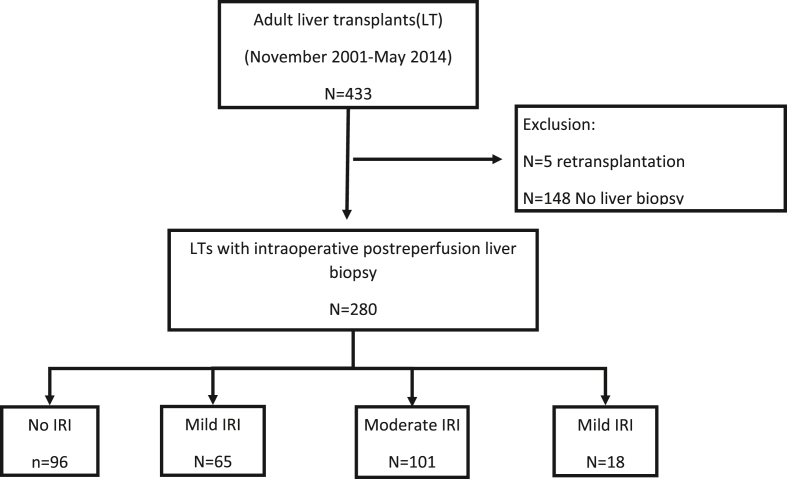
Results: We included 280 OLTs (64.7%). The histopathological assessment of IRI severity was as follows: no IRI (N = 96, 34.3%), mild IRI (N = 65; 23.2%), moderate IRI (N = 101; 36.1%), and severe IRI (N = 18; 6.4%). The incidence rates of initial good graft function (IGGF), primary nonfunction and early allograft dysfunction (EAD) were 32.5%, 3.9%, and 18.6%, respectively. Severe IRI was associated with a lower incidence of IGGF (OR: 0.34, 95% CI 0.12-0.92; P = 0.03). Patients with severe IRI tended to have a higher incidence of EAD (33.2% vs. 18.6, P = 0.23). The cold ischemia time was an independent predictor of severe IRI on the multivariate analysis. Severe IRI was associated with poor 1- and 5-year overall survival rates (67% and 44%, respectively, compared with 84 and 68% in nonsevere IRI). Patients with severe IRI exhibited worse graft and overall survival.
Conclusions: Cold ischemia time predicts the development of severe IRI. Patients with severe IRI show worse graft and overall survival and a lower incidence of IGGF, suggesting that histopathological findings could be useful for identifying patients at high risk of worse outcomes after OLT.
Keywords: ALD, alcohol-related liver disease; ALF, acute liver failure; ALT, alanine aminotransferase; CIHD, chronic ischaemic heart disease; CNI, calcineurin inhibitors; COPD, chronic obstructive pulmonary disease; DBD, donation after brain death; EAD, early allograft dysfunction; H&E, hematoxylin and eosin; HBV, hepatitis B virus; HCC, hepatocellular carcinoma; HCV, hepatitis C virus; IGGF, initial good graft function; IQR, interquartile range; IRI, ischaemia/reperfusion injury; MELD, Model for End-stage Liver Disease; OLT, orthotopic liver transplantation; ONT, Organización Nacional de Transplantes; PBC, primary biliary cholangitis; PNF, primary nonfunction; PRB, postreperfusion liver biopsy; SD, standard deviation; STROBE, Strengthening the Reporting of Observational studies in Epidemiology; cold ischemia time; early allograft dysfunction; ischemia reperfusion injury; liver transplantation; postreperfusion biopsy.
© 2021 Indian National Association for Study of the Liver. Published by Elsevier B.V. All rights reserved.
Figures


Similar articles
-
Advancements in Predictive Tools for Primary Graft Dysfunction in Liver Transplantation: A Comprehensive Review.J Clin Med. 2024 Jun 27;13(13):3762. doi: 10.3390/jcm13133762. J Clin Med. 2024. PMID: 38999328 Free PMC article. Review.
-
Procalcitonin in early allograft dysfunction after orthotopic liver transplantation: a retrospective single centre study.BMC Gastroenterol. 2022 Aug 31;22(1):404. doi: 10.1186/s12876-022-02486-5. BMC Gastroenterol. 2022. PMID: 36045337 Free PMC article.
-
Effect of Donor Hepatic Steatosis on Ischemia Reperfusion Injury in Liver Transplant Recipient.J Clin Exp Hepatol. 2020 May-Jun;10(3):236-244. doi: 10.1016/j.jceh.2019.07.004. Epub 2019 Jul 12. J Clin Exp Hepatol. 2020. PMID: 32405180 Free PMC article.
-
Analysis of ischemia/reperfusion injury in time-zero biopsies predicts liver allograft outcomes.Liver Transpl. 2015 Apr;21(4):487-99. doi: 10.1002/lt.24072. Liver Transpl. 2015. PMID: 25545865
-
Intraoperative Anesthetic Strategies to Mitigate Early Allograft Dysfunction After Orthotopic Liver Transplantation: A Narrative Review.Anesth Analg. 2024 Dec 1;139(6):1267-1282. doi: 10.1213/ANE.0000000000006902. Epub 2024 Mar 5. Anesth Analg. 2024. PMID: 38442076 Review.
Cited by
-
Hedgehog costimulation during ischemia-reperfusion injury potentiates cytokine and homing responses of CD4+ T cells.Front Immunol. 2023 Oct 17;14:1248027. doi: 10.3389/fimmu.2023.1248027. eCollection 2023. Front Immunol. 2023. PMID: 37915586 Free PMC article.
-
Advancements in Predictive Tools for Primary Graft Dysfunction in Liver Transplantation: A Comprehensive Review.J Clin Med. 2024 Jun 27;13(13):3762. doi: 10.3390/jcm13133762. J Clin Med. 2024. PMID: 38999328 Free PMC article. Review.
-
The Coming Age of Antisense Oligos for the Treatment of Hepatic Ischemia/Reperfusion (IRI) and Other Liver Disorders: Role of Oxidative Stress and Potential Antioxidant Effect.Antioxidants (Basel). 2024 May 31;13(6):678. doi: 10.3390/antiox13060678. Antioxidants (Basel). 2024. PMID: 38929116 Free PMC article. Review.
References
-
- Ahmed A., Keeffe E.B. Current indications and contraindications for liver transplantation. Clin Liver Dis. 2007 May;11:227–247. - PubMed
-
- Chen X.B., Xu M.Q. Primary graft dysfunction after liver transplantation. Hepatobiliary Pancreat Dis Int. 2014 Apr;13:125–137. - PubMed
-
- Uemura T., Randall H.B., Sanchez E.Q., et al. Liver retransplantation for primary nonfunction: analysis of a 20-year single-center experience. Liver Transpl. 2007 Feb;13:227–233. - PubMed
-
- Neves D.B., Rusi M.B., Diaz L.G.G., Salvalaggio P. Primary graft dysfunction of the liver: definitions, diagnostic criteria and risk factors. Einstein (Sao Paulo) 2016;14:567–572. - PubMed
-
- Olthoff K.M., Kulik L., Samstein B., et al. Validation of a current definition of early allograft dysfunction in liver transplant recipients and analysis of risk factors. Liver Transplant. 2010 Aug;16:943–949. - PubMed
LinkOut - more resources
Full Text Sources
