

Management of Portal Hypertension
- PMID: 35814519
- PMCID: PMC9257868
- DOI: 10.1016/j.jceh.2022.03.002
Management of Portal Hypertension
Abstract
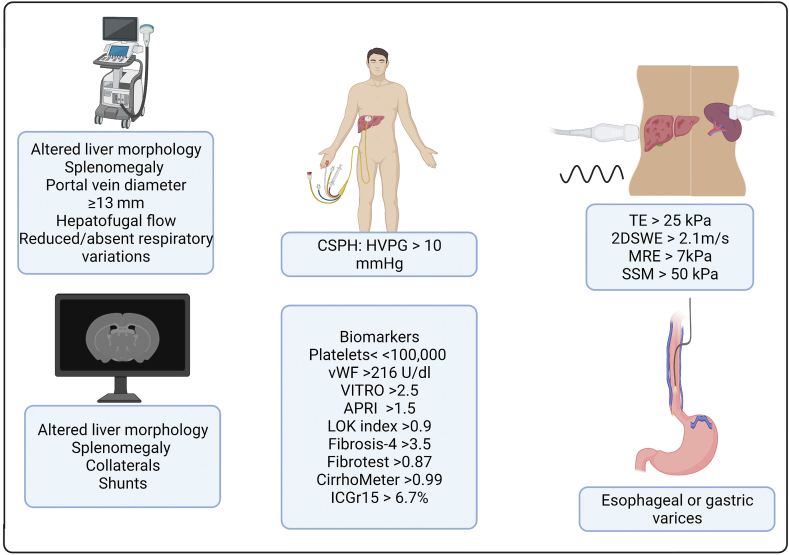
Portal hypertension is the cause of the clinical complications associated with cirrhosis. The primary complications of portal hypertension are ascites, acute variceal bleed, and hepatic encephalopathy. Hepatic venous pressure gradient measurement remains the gold standard test for diagnosing cirrhosis-related portal hypertension. Hepatic venous pressure gradient more than 10 mmHg is associated with an increased risk of complications and is termed clinically significant portal hypertension (CSPH). Clinical, laboratory, and imaging methods can also aid in diagnosing CSPH non-invasively. Recently, deep learning methods have been demonstrated to diagnose CSPH effectively. The management of portal hypertension is always individualized and is dependent on the etiology, the availability of therapies, and the degree of portal hypertension complications. In this review, we discuss the diagnosis and management of cirrhosis-related portal hypertension in detail. Also, we highlight the history of portal hypertension and future research areas in portal hypertension.
Keywords: ACLF, acute-on-chronic liver failure; AKI, acute kidney injury; APRI, AST to platelet ratio; AST, aspartate transaminase; BB, Beta blocker; BRTO, balloon occluded retrograde transvenous obliteration; CKD, chronic kidney disease; CSPH, clinically significant portal hypertension; CT, computed tomography; GFR, glomerular filtration rate; GOV, gastrpoesopahegal varices; HE, hepatic encephalopathy; HRS, hepatorenal syndrome; HVPG, hepatic venous pressure gradient; ICG, indocyanine green; LOLA, l-ornithine l-aspartate; NAFLD, Non-alcoholic fatty liver disease; SBP, spontaneous bacterial peritonitis; SGLT2I, sodium glucose co-transporter 2 inhibitors; SSM, splenic stiffness measurement; TE, transient elastography; TIPS, transjugular intrahepatic portosystemic shunt; VITRO, von Willebrand factor to platelet counts; acute kidney injury; ascites; hemodynamics; history; vasoconstrictors.
© 2022 Indian National Association for Study of the Liver. Published by Elsevier B.V. All rights reserved.
Figures

References
-
- de Franchis R. Expanding consensus in portal hypertension: report of the Baveno VI Consensus Workshop: stratifying risk and individualizing care for portal hypertension. J Hepatol. 2015;63:743–752. - PubMed
-
- Ripoll C., Groszmann R., Garcia-Tsao G., et al. Hepatic venous pressure gradient predicts clinical decompensation in patients with compensated cirrhosis. Gastroenterology. 2007;133:481–488. - PubMed
-
- Garcia-Tsao G., Abraldes J.G., Berzigotti A., Bosch J. Portal hypertensive bleeding in cirrhosis: risk stratification, diagnosis, and management: 2016 practice guidance by the American Association for the study of liver diseases. Hepatology. 2017;65:310–335. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
