

The impact of government- and institution-implemented COVID-19 control measures on tertiary- and regional-level intensive care units in Pietermaritzburg, KwaZulu-Natal Province, South Africa
- PMID: 35814623
- PMCID: PMC9252134
- DOI: 10.7196/SAJCC.2022.v38i1.515
The impact of government- and institution-implemented COVID-19 control measures on tertiary- and regional-level intensive care units in Pietermaritzburg, KwaZulu-Natal Province, South Africa
Abstract
Background: The COVID-19 pandemic has had a significant impact on healthcare systems globally as most countries were not equipped to deal with the outbreak. To avoid complete collapse of intensive care units (ICUs) and health systems as a whole, containment measures had to be instituted. In South Africa (SA), the biggest intervention was the government-regulated national lockdown instituted in March 2020.
Objectives: To evaluate the effects of the implemented lockdown and institutional guidelines on the admission rate and profile of non-COVID-19 patients in a regional and tertiary level ICU in Pietermaritzburg, KwaZulu-Natal Province, SA.
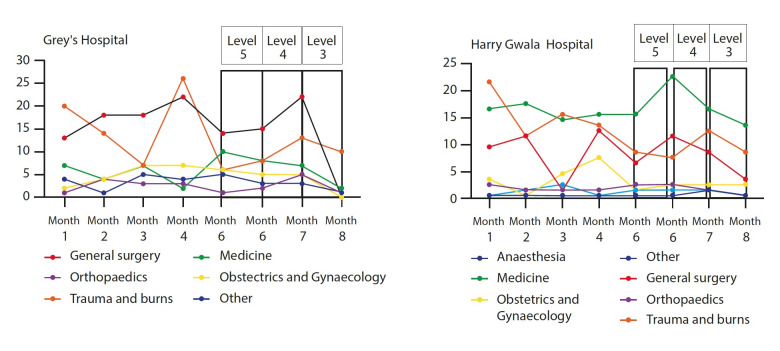
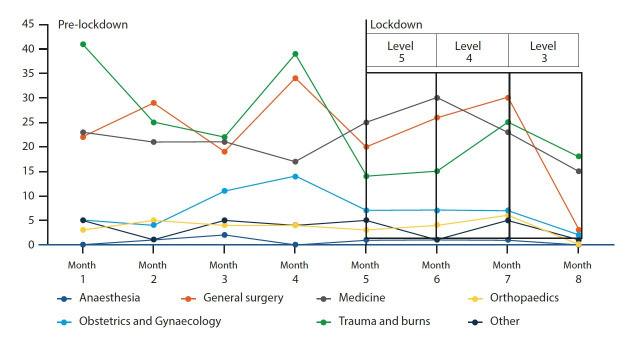
Methods: A retrospective analysis of all non-COVID-19 admissions to Harry Gwala and Greys hospitals was performed over an 8-month period (1 December 2019 - 31 July 2020), which included 4 months prior to lockdown implementation and 4 months post lockdown.
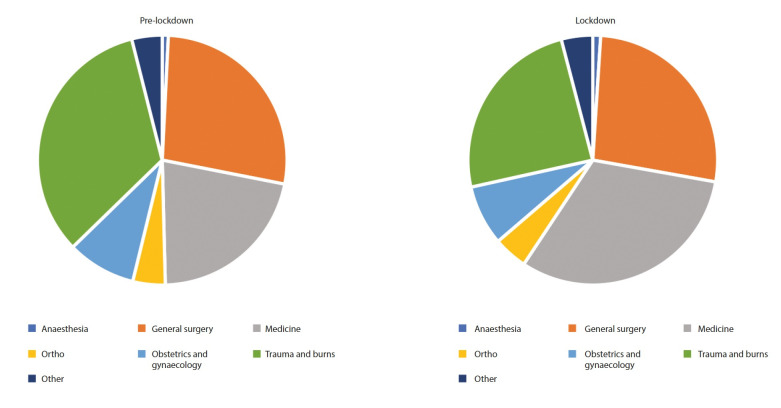
Results: There were a total of 678 non-COVID-19 admissions over the 8-month period. The majority of the admissions were at Greys Hospital (52.4%; n=355) and the rest at Harry Gwala Hospital (47.6%; n=323). A change in spectrum of patients admitted was noted, with a significant decrease in trauma and burns admissions post lockdown implementation (from 34.2 - 24.6%; p=0.006). Conversely, there was a notable increase in non-COVID-19 medical admissions after lockdown regulations were implemented (20.1 - 31.3%; p<0.001). We hypothesised that this was due to the gap left by trauma patients in an already overburdened system.
Conclusion: Despite the implementation of a national lockdown and multiple institutional directives, there was no significant decrease in the total number of non-COVID-19 admissions to ICUs. There was, however, a notable change in spectrum of patients admitted, which may reflect a bias towards trauma admissions in the pre COVID-19 era.
Contributions of the study: We describe the impact of the COVID-19 pandemic on critical care services in a resource-limited setting. We also demonstrate the ongoing need for intensive care unit beds within the public sector.
Keywords: COVID-19; ICU; lockdown; non-COVID-19 admissions.
Conflict of interest statement
Conflicts of interest: None.
Figures
References
-
- Morris D, Rogers M, Kissmer N, et al. Impact of lockdown measures implemented during the COVID-19 pandemic on the burden of trauma presentations to a regional emergency department in Kwa-Zulu Natal, South Africa. African J Emergency Med. 2020;10(4):193–196. doi: 10.1016/j.afjem.2020.06.005. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous