

Profile of the Lower Respiratory Tract Microbiome in Human Immunodeficiency Virus/Acquired Immunodeficiency Syndrome and Lung Disease
- PMID: 35814692
- PMCID: PMC9260662
- DOI: 10.3389/fmicb.2022.888996
Profile of the Lower Respiratory Tract Microbiome in Human Immunodeficiency Virus/Acquired Immunodeficiency Syndrome and Lung Disease
Abstract
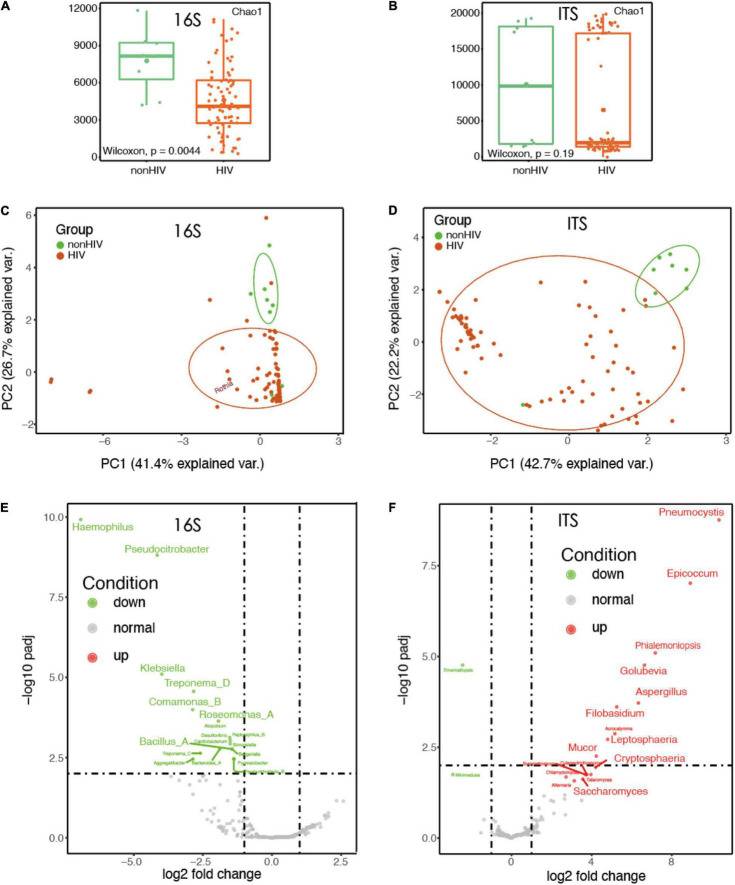
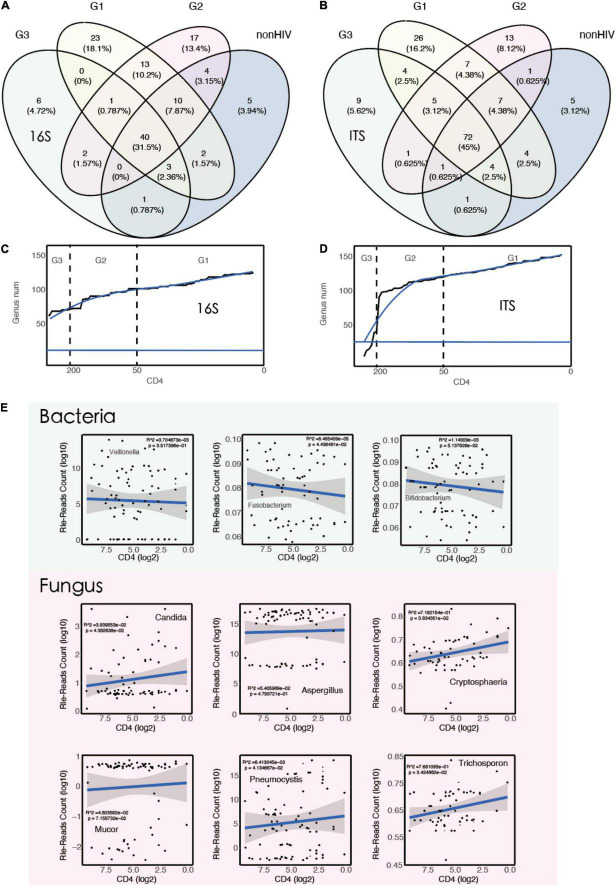
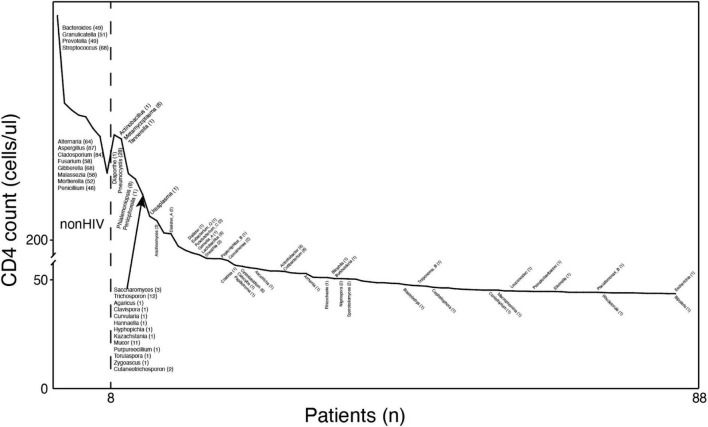
Once an human immunodeficiency virus (HIV)-infected individual enters the onset period, a variety of opportunistic infections may occur, affecting various systems and organs throughout the body, due to the considerable reduction in the body's immune function. The objectives of this study were to explore the relationship between immune status and microbial communities in the lungs of individuals with HIV infection. A total of 88 patients with lung disease [80 (91%) HIV-positive and 8 (9%) HIV-negative] were enrolled in our study between January and July 2018, and 88 bronchoalveolar lavage fluid (BALF) samples were obtained during bronchoscopy. In this cross-sectional study, we investigated differences in the pulmonary microbiome of patients with HIV who had different immune statuses. The diversity of bacteria in the lungs of HIV-positive individuals was lower than that in HIV-negative individuals (p < 0.05). There was a significant difference in the composition and distribution of bacteria and fungi between the HIV-positive and HIV-negative groups (p < 0.01). The number of fungal species in the BALF of HIV-positive patients was higher than in HIV-negative patients. The diversity of bacteria and fungi in the BALF of HIV-positive patients increased with decreasing CD4 T-cell counts. Linear regression analysis showed that Pneumocystis (R 2 = 6.4e-03, p < 0.05), Cryptosphaeria (R 2 = 7.2e-01, p < 0.05), Candida (R 2 = 3.9e-02, p < 0.05), and Trichosporon (R 2 = 7.7e-01, p < 0.05) were negatively correlated with CD4 counts (F-test, p < 0.05). The samples collected from HIV-positive patients exhibited a different pattern relative to those from the HIV-negative group. Differences in host immune status cause differences in the diversity and structure of lower respiratory tract microorganisms.
Keywords: CD4; HIV; bronchoalveolar lavage; lower respiratory tract; microbiota; next-generation sequencing.
Copyright © 2022 Chen, Tian, Wang, Zhao, Chen and Zhang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
[Deep lung--cellular reaction to HIV].Rev Port Pneumol. 2007 Mar-Apr;13(2):175-212. Rev Port Pneumol. 2007. PMID: 17492233 Review. Portuguese.
-
Enhanced in vivo human immunodeficiency virus-1 replication in the lungs of human immunodeficiency virus-infected persons with Pneumocystis carinii pneumonia.Am J Respir Crit Care Med. 1999 Dec;160(6):2048-55. doi: 10.1164/ajrccm.160.6.9902099. Am J Respir Crit Care Med. 1999. PMID: 10588627
-
Salivary microbial diversity at different stages of human immunodeficiency virus infection.Microb Pathog. 2021 Jun;155:104913. doi: 10.1016/j.micpath.2021.104913. Epub 2021 Apr 27. Microb Pathog. 2021. PMID: 33915204
-
Correlation of the lung microbiota with metabolic profiles in bronchoalveolar lavage fluid in HIV infection.Microbiome. 2016 Jan 20;4:3. doi: 10.1186/s40168-016-0147-4. Microbiome. 2016. PMID: 26792212 Free PMC article.
-
Lung microbiome in human immunodeficiency virus infection.Transl Res. 2017 Jan;179:97-107. doi: 10.1016/j.trsl.2016.07.008. Epub 2016 Jul 18. Transl Res. 2017. PMID: 27496318 Free PMC article. Review.
Cited by
-
Alterations in circulating markers in HIV/AIDS patients with poor immune reconstitution: Novel insights from microbial translocation and innate immunity.Front Immunol. 2022 Oct 17;13:1026070. doi: 10.3389/fimmu.2022.1026070. eCollection 2022. Front Immunol. 2022. PMID: 36325329 Free PMC article. Review.
-
Immunoregulatory role of pulmonary microbiota in lung cancer: a bibliometric analysis.Discov Oncol. 2025 Jun 11;16(1):1054. doi: 10.1007/s12672-025-02595-z. Discov Oncol. 2025. PMID: 40498209 Free PMC article.
References
-
- Balaan M. R. (1990). Pneumocystis carinii pneumonia. W V Med J. Dec 86 561–565. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials