

Dietary factors that affect the risk of pre-eclampsia
- PMID: 35814725
- PMCID: PMC9237898
- DOI: 10.1136/bmjnph-2021-000399
Dietary factors that affect the risk of pre-eclampsia
Abstract
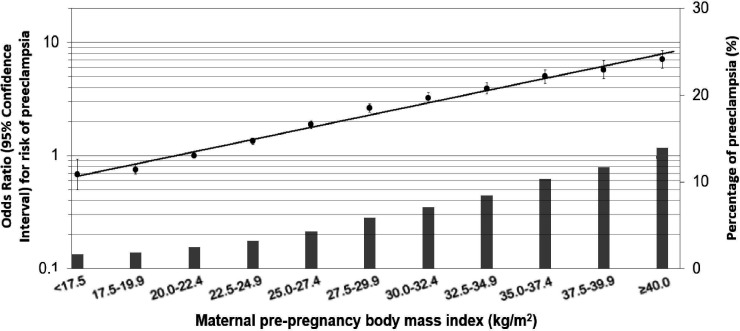
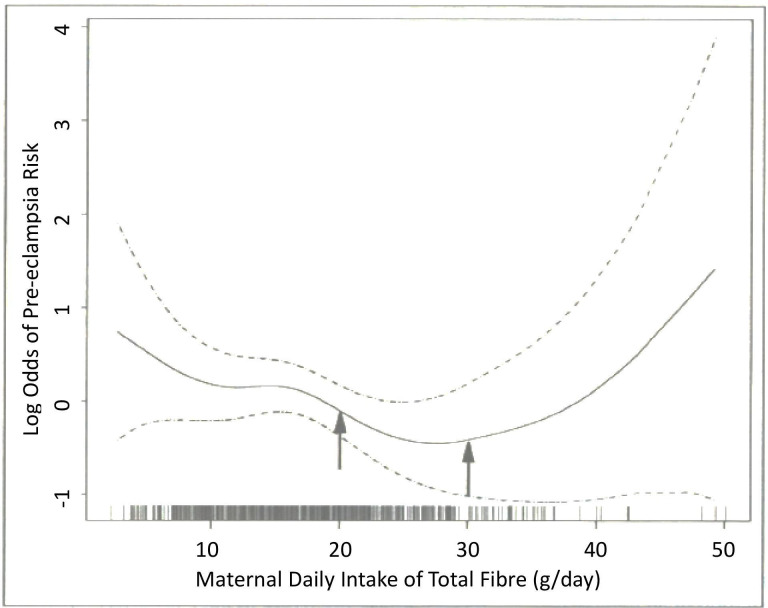
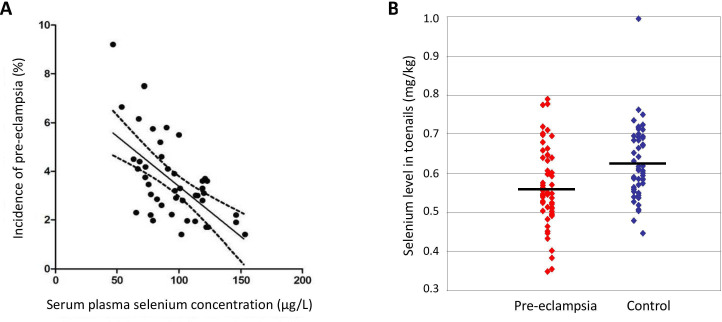
Pre-eclampsia affects 3%-5% of pregnant women worldwide and is associated with a range of adverse maternal and fetal outcomes, including maternal and/or fetal death. It particularly affects those with chronic hypertension, pregestational diabetes mellitus or a family history of pre-eclampsia. Other than early delivery of the fetus, there is no cure for pre-eclampsia. Since diet or dietary supplements may affect the risk, we have carried out an up-to-date, narrative literature review to assess the relationship between nutrition and pre-eclampsia. Several nutrients and dietary factors previously believed to be implicated in the risk of pre-eclampsia have now been shown to have no effect on risk; these include vitamins C and E, magnesium, salt, ω-3 long-chain polyunsaturated fatty acids (fish oils) and zinc. Body mass index is proportionally correlated with pre-eclampsia risk, therefore women should aim for a healthy pre-pregnancy body weight and avoid excessive gestational and interpregnancy weight gain. The association between the risk and progression of the pathophysiology of pre-eclampsia may explain the apparent benefit of dietary modifications resulting from increased consumption of fruits and vegetables (≥400 g/day), plant-based foods and vegetable oils and a limited intake of foods high in fat, sugar and salt. Consuming a high-fibre diet (25-30 g/day) may attenuate dyslipidaemia and reduce blood pressure and inflammation. Other key nutrients that may mitigate the risk include increased calcium intake, a daily multivitamin/mineral supplement and an adequate vitamin D status. For those with a low selenium intake (such as those living in Europe), fish/seafood intake could be increased to improve selenium intake or selenium could be supplemented in the recommended multivitamin/mineral supplement. Milk-based probiotics have also been found to be beneficial in pregnant women at risk. Our recommendations are summarised in a table of guidance for women at particular risk of developing pre-eclampsia.
Keywords: blood pressure lowering; dietary patterns; nutrient deficiencies; nutritional treatment; weight management.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources