

Serum Total Bilirubin With Hospital Survival in Adults During Extracorporeal Membrane Oxygenation
- PMID: 35814759
- PMCID: PMC9263081
- DOI: 10.3389/fmed.2022.914557
Serum Total Bilirubin With Hospital Survival in Adults During Extracorporeal Membrane Oxygenation
Abstract
Background: Extracorporeal membrane oxygenation (ECMO) is widely used for refractory cardiopulmonary failure treatment. The disadvantage of ECMO is its higher risk profile and clinical resource consumption. This observation examines the role of serum total bilirubin (TBIL) as a predictor of adult patient outcomes on ECMO support.
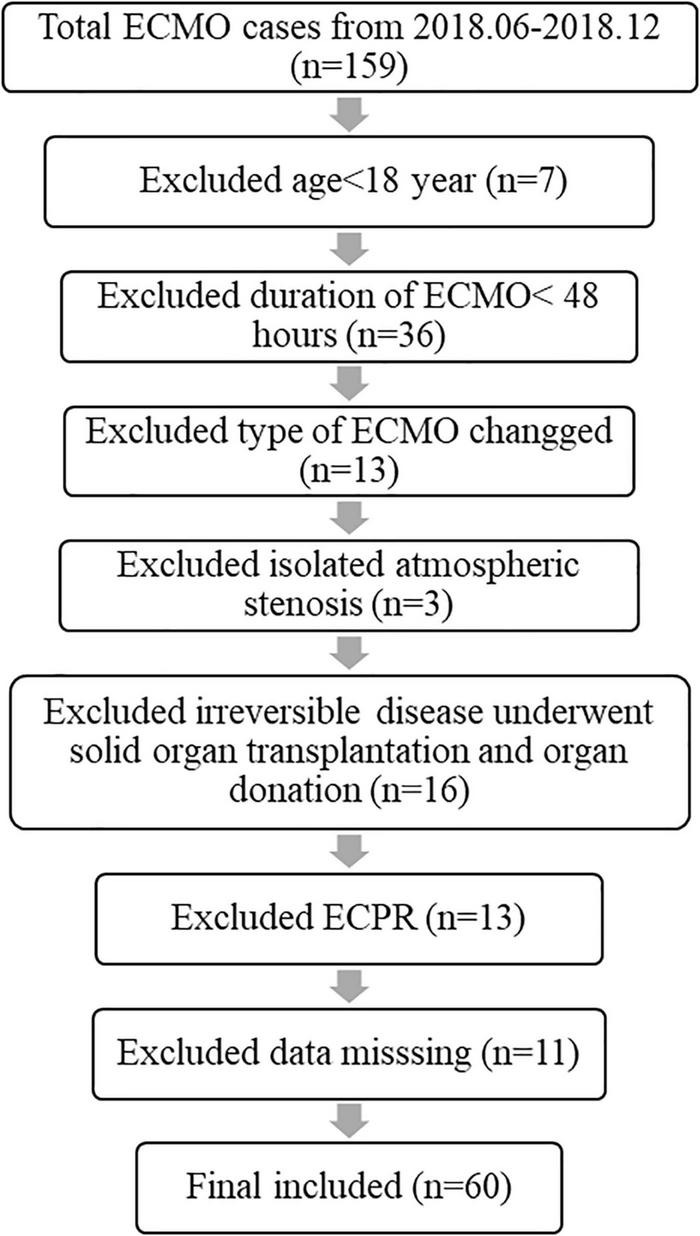
Methods: This retrospective observation reports a single-center experience with adults on ECMO support between 2018 and 2021. Data were collected regarding demographics, ECMO details, laboratory parameters, and outcomes. We examined the elevation of TBIL to predict survival and variables associated with hyperbilirubinemia.
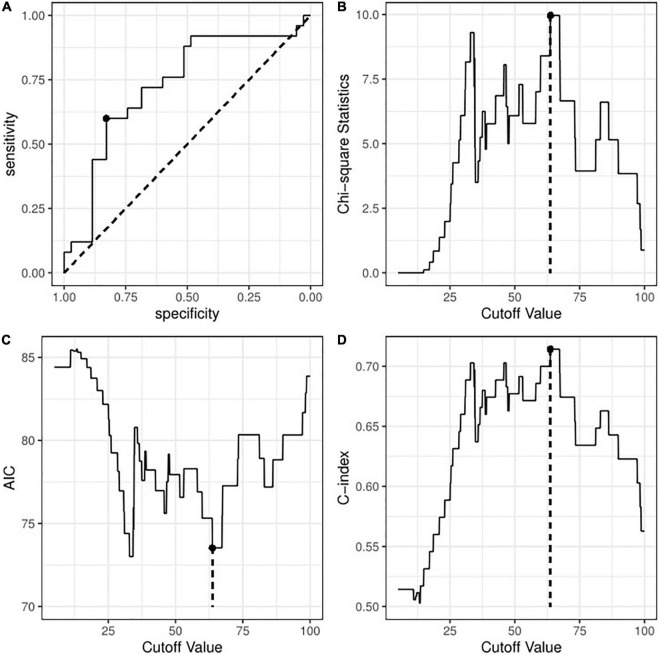
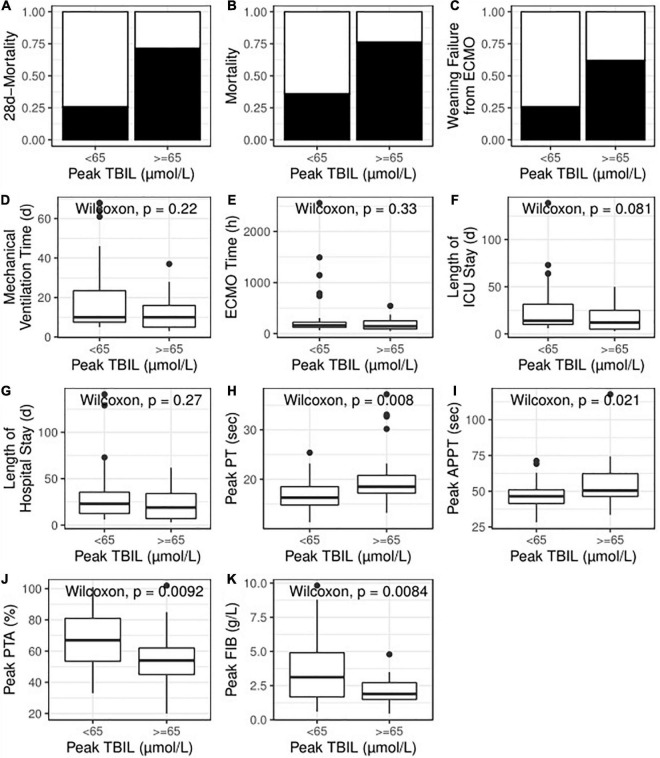
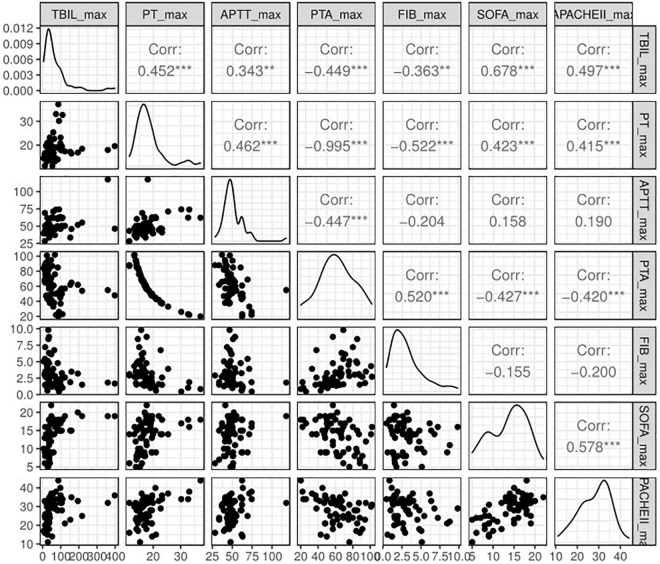
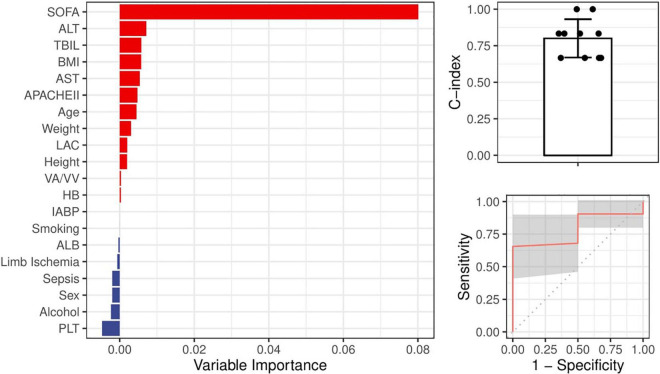
Results: The patients who died within 28 days had a twofold higher peak level of TBIL than those who survived [73.10 (38.60, 98.64) vs. 34.50 (24.03, 54.85); P = 0.003]. Univariate logistic regression analyses demonstrated that high TBIL was remarkably associated with an elevated risk of 28-day mortality (OR: 7.25; 95% CI: 2.31-25.49; P = 0.001) and total mortality (OR: 5.71; 95% CI: 1.82-20.66; P = 0.001). The TBIL value was 65 μmol/L as the best cut-off value, and the observation group was divided into a high TBIL subgroup (n = 21) or a low TBIL subgroup (n = 39). The demographic and clinical features did not show a difference, whereas Sequential Organ Failure Assessment (SOFA) and APACHE II scores and ALT, AST, and LAC before ECMO initiation correlated with high or low TBIL (P < 0.05). For coagulation function at the time of TBIL peak, the levels of prothrombin time (PT), activated partial thromboplastin time (APTT), prothrombin time activity (PTA), and fibrinogen (FIB) were different between the two subgroups (P < 0.05). The SOFA score was potentially associated with hyperbilirubinemia after ECMO initiation, and the prediction accuracy was 0.800.
Conclusion: Serum total bilirubin elevation appears after ECMO initiation and correlates with survival, while other markers of liver injury do not. Serum total bilirubin is an easy-to-measure biomarker to be a predictor of survival after ECMO initiation.
Keywords: extracorporeal membrane oxygenation; hyperbilirubinemia; prognosis; survival; total bilirubin.
Copyright © 2022 Huang, Shao, Zhang, Fang, Jin, Han and Liu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Comment in
-
Commentary: Serum total bilirubin with hospital survival in adults during extracorporeal membrane oxygenation.Front Med (Lausanne). 2022 Sep 28;9:1022207. doi: 10.3389/fmed.2022.1022207. eCollection 2022. Front Med (Lausanne). 2022. PMID: 36250096 Free PMC article. No abstract available.
Similar articles
-
Incidence, Risk Factors, and Outcomes of Hyperbilirubinemia in Adult Cardiac Patients Supported by Veno-Arterial ECMO.Artif Organs. 2018 Feb;42(2):148-154. doi: 10.1111/aor.12979. Epub 2017 Sep 6. Artif Organs. 2018. PMID: 28877352
-
[Correlation between model for end-stage liver disease score and prognosis in mushroom poisoning patients: a multicenter clinical study].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2018 Jan;30(1):67-71. doi: 10.3760/cma.j.issn.2095-4352.2018.01.013. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2018. PMID: 29308761 Chinese.
-
[Prognostic value of oxygen challenge test for patients with cardiogenic shock receiving extracorporeal membrane oxygenation].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2017 Dec;29(12):1102-1106. doi: 10.3760/cma.j.issn.2095-4352.2017.12.010. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2017. PMID: 29216944 Chinese.
-
[Analysis of risk factors for prognosis of patients with acute paraquat intoxication].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2015 Nov;27(11):906-10. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2015. PMID: 27132458 Chinese.
-
[Predictive values of different critical scoring systems for survival rate after discharge in critically ill patients supported by extracorporeal membrane oxygenation].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2018 May;30(5):456-460. doi: 10.3760/cma.j.issn.2095-4352.2018.05.012. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2018. PMID: 29764551 Chinese.
Cited by
-
Risk factors and prognostic modeling in bridging extracorporeal membrane oxygenation patients before lung transplantation.J Thorac Dis. 2024 Aug 31;16(8):5238-5247. doi: 10.21037/jtd-24-430. Epub 2024 Aug 23. J Thorac Dis. 2024. PMID: 39268095 Free PMC article.
-
Association between PT, PT-INR, and in-hospital mortality in critically ill patients with tumors: A retrospective cohort study.Front Public Health. 2023 Mar 21;11:1036463. doi: 10.3389/fpubh.2023.1036463. eCollection 2023. Front Public Health. 2023. PMID: 37026132 Free PMC article.
-
Commentary: Serum total bilirubin with hospital survival in adults during extracorporeal membrane oxygenation.Front Med (Lausanne). 2022 Sep 28;9:1022207. doi: 10.3389/fmed.2022.1022207. eCollection 2022. Front Med (Lausanne). 2022. PMID: 36250096 Free PMC article. No abstract available.
-
ECMO Retrieval Program: What Have We Learned So Far.Life (Basel). 2023 Jan 5;13(1):157. doi: 10.3390/life13010157. Life (Basel). 2023. PMID: 36676106 Free PMC article.
-
Anticoagulation and associated complications in veno-arterial extracorporeal membrane oxygenation in adult patients: A systematic review and meta-analysis.Crit Care Resusc. 2024 Nov 26;26(4):332-363. doi: 10.1016/j.ccrj.2024.10.003. eCollection 2024 Dec. Crit Care Resusc. 2024. PMID: 39781486 Free PMC article. Review.
References
LinkOut - more resources
Full Text Sources