

Purely endoscopic appendectomy
- PMID: 35815161
- PMCID: PMC9264142
- DOI: 10.1016/j.vgie.2022.03.010
Purely endoscopic appendectomy
Abstract
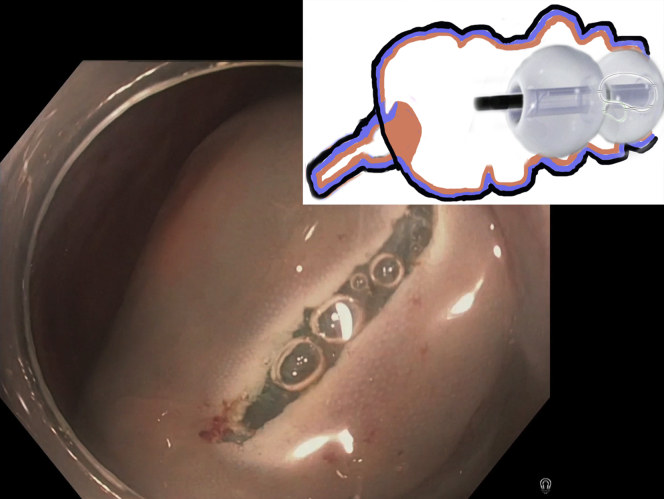
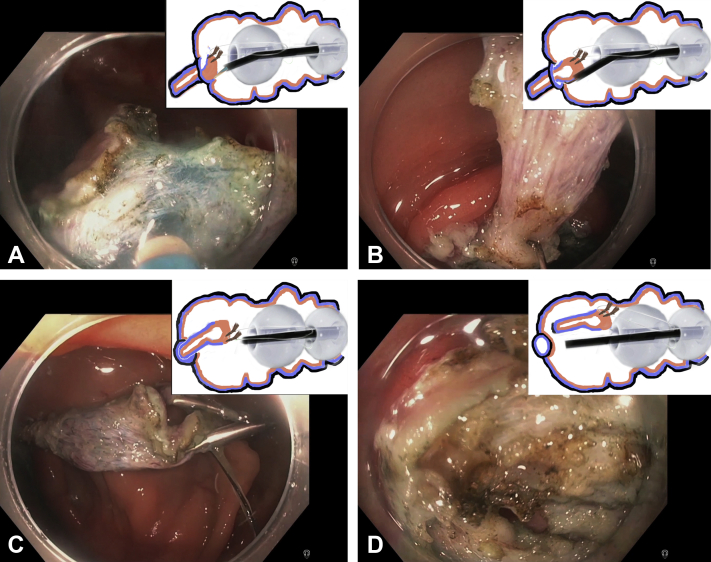
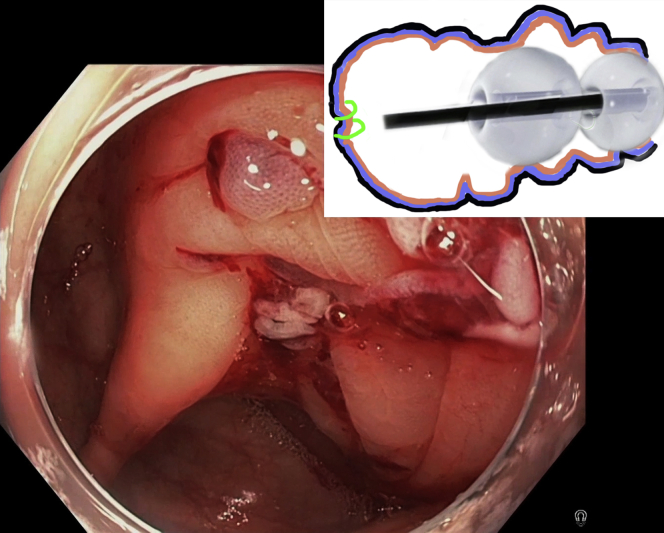
Video 1Submucosal nodule in the cecum. After submucosal injection, a circumferential incision of the mucosa surrounding the lesion is performed with DualKnife (Olympus America, Center Valley, Pa, USA). The fore-balloon of the double-balloon endoluminal interventional platform (DBEIP) is deployed and the edges of the circumferential incision are attached with 2 endoscopic clips to the long suture-loop mounted on the fore-balloon of the DBEIP. The fore-balloon is retracted in anal direction, pulling the lesion into the cecum. Careful endoscopic submucosal dissection is performed with DualKnife and HookKnife (Olympus America). Dissection is markedly facilitated by traction and continued until the entire appendix is pulled into the cecum. The tip of the appendix is separated from surrounding tissues, resulting in a full-thickness cecal wall defect. The suture-loop holding the resected appendix is cut with LoopCutter (Olympus America). The resected appendix is removed through DBEIP and the Overstitch endoscopic suturing device (Apollo Endosurgery, Austin, Tex, USA) is advanced into the cecum. The full-thickness defect in the cecal wall is completely closed with 2 continuous sutures. The final view demonstrates the entire resected appendix.
Keywords: DBEIP, double-balloon endoluminal interventional platform.
© 2022 American Society for Gastrointestinal Endoscopy. Published by Elsevier Inc.
Figures




References
-
- Dotai T., Coker A.M., Antozzi L., et al. Transgastric large-organ extraction: the initial human experience. Surg Endosc. 2013;27:394–399. - PubMed
-
- Auyang E.D., Santos B.F., Enter D.H., et al. Natural orifice translumenal endoscopic surgery (NOTES®): a technical review. Surg Endosc. 2011;25:3135–3148. - PubMed
-
- Palanivelu C., Rajan P.S., Rangarajan M., et al. Transvaginal endoscopic appendectomy in humans: a unique approach to NOTES-world's first report. Surg Endosc. 2008;22:1343–1347. - PubMed
LinkOut - more resources
Full Text Sources
