

Assessment of Racial and Ethnic Differences in Oxygen Supplementation Among Patients in the Intensive Care Unit
- PMID: 35816344
- PMCID: PMC9274443
- DOI: 10.1001/jamainternmed.2022.2587
Assessment of Racial and Ethnic Differences in Oxygen Supplementation Among Patients in the Intensive Care Unit
Abstract
Importance: Pulse oximetry (SpO2) is routinely used for transcutaneous monitoring of blood oxygenation, but it can overestimate actual oxygenation. This is more common in patients of racial and ethnic minority groups. The extent to which these discrepancies are associated with variations in treatment is not known.
Objective: To determine if there are racial and ethnic disparities in supplemental oxygen administration associated with inconsistent pulse oximeter performance.
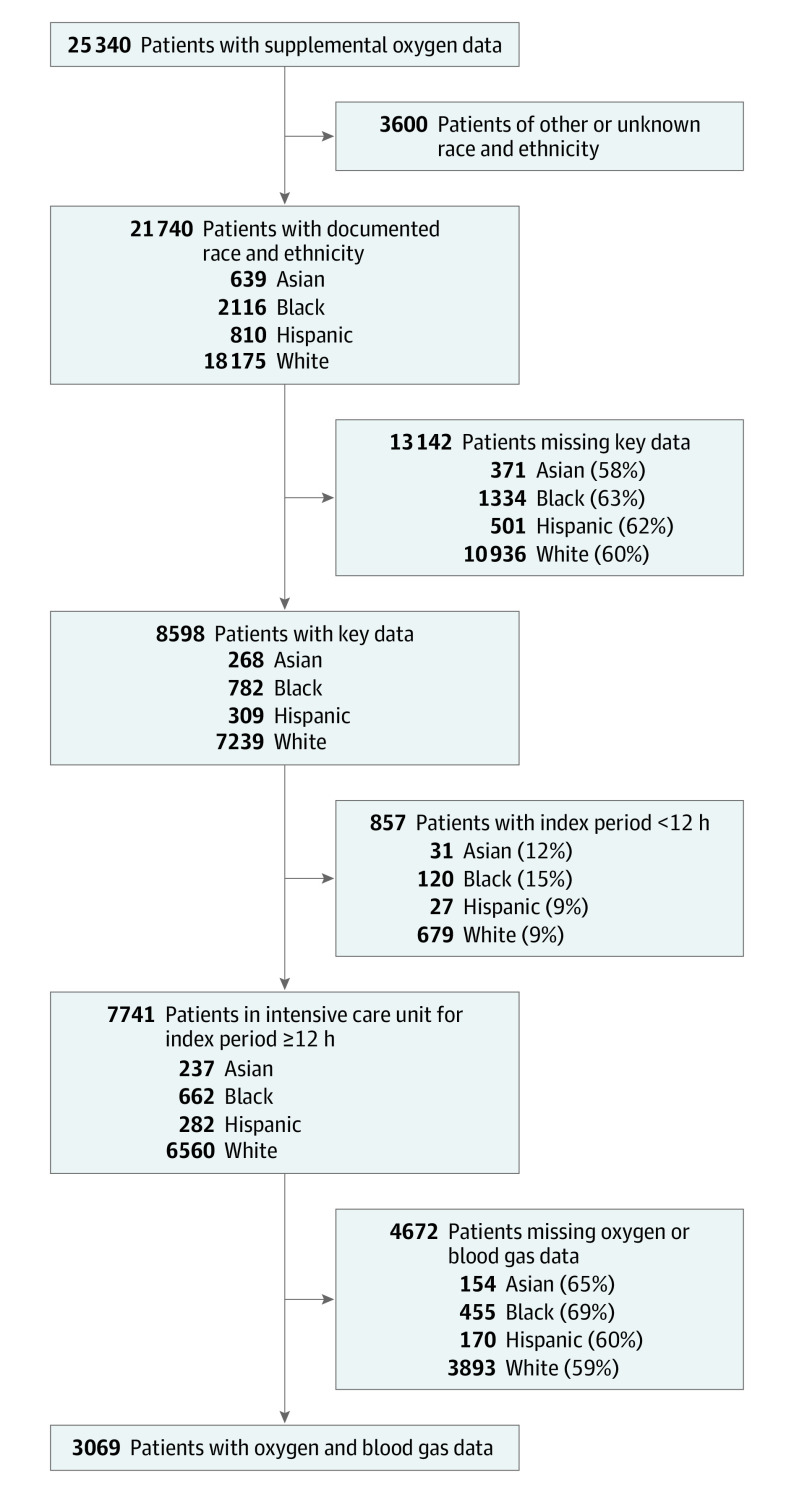
Design, setting, and participants: This retrospective cohort study was based on the Medical Information Mart for Intensive Care (MIMIC)-IV critical care data set. Included patients were documented with a race and ethnicity as Asian, Black, Hispanic, or White and were admitted to the intensive care unit (ICU) for at least 12 hours before needing advanced respiratory support, if any. Oxygenation levels and nasal cannula flow rates for up to 5 days from ICU admission or until the time of intubation, noninvasive positive pressure ventilation, high-flow nasal cannula, or tracheostomy were analyzed.
Main outcomes and measures: The primary outcome was time-weighted average supplemental oxygen rate. Covariates included race and ethnicity, sex, SpO2-hemoglobin oxygen saturation discrepancy, data duration, number and timing of blood gas tests on ICU days 1 to 3, partial pressure of carbon dioxide, hemoglobin level, average respiratory rate, Elixhauser comorbidity scores, and need for vasopressors or inotropes.
Results: This cohort included 3069 patients (mean [SD] age, 66.9 [13.5] years; 83 were Asian, 207 were Black, 112 were Hispanic, 2667 were White). In a multivariable linear regression, Asian (coefficient, 0.602; 95% CI, 0.263 to 0.941; P = .001), Black (coefficient, 0.919; 95% CI, 0.698 to 1.140; P < .001), and Hispanic (coefficient, 0.622; 95% CI, 0.329 to 0.915; P < .001) race and ethnicity were all associated with a higher SpO2 for a given hemoglobin oxygen saturation. Asian (coefficient, -0.291; 95% CI, -0.546 to -0.035; P = .03), Black (coefficient, -0.294; 95% CI, -0.460 to -0.128; P = .001), and Hispanic (coefficient, -0.242; 95% CI, -0.463 to -0.020; P = .03) race and ethnicity were associated with lower average oxygen delivery rates. When controlling for the discrepancy between average SpO2 and average hemoglobin oxygen saturation, race and ethnicity were not associated with oxygen delivery rate. This discrepancy mediated the effect of race and ethnicity (-0.157; 95% CI, -0.250 to -0.057; P = .002).
Conclusions and relevance: In this cohort study, Asian, Black, and Hispanic patients received less supplemental oxygen than White patients, and this was associated with differences in pulse oximeter performance, which may contribute to known race and ethnicity-based disparities in care.
Conflict of interest statement
Figures

Comment in
-
Confronting the Clinical Implications of Racial and Ethnic Discrepancy in Pulse Oximetry.JAMA Intern Med. 2022 Aug 1;182(8):858. doi: 10.1001/jamainternmed.2022.2581. JAMA Intern Med. 2022. PMID: 35816351 No abstract available.
-
Ensuring Progress Toward Racial Equity in Pulse Oximetry-Reply.JAMA Intern Med. 2022 Dec 1;182(12):1329-1330. doi: 10.1001/jamainternmed.2022.4857. JAMA Intern Med. 2022. PMID: 36342690 No abstract available.
-
Ensuring Progress Toward Racial Equity in Pulse Oximetry.JAMA Intern Med. 2022 Dec 1;182(12):1329. doi: 10.1001/jamainternmed.2022.4854. JAMA Intern Med. 2022. PMID: 36342695 No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
