

Efficacy and Safety of Elexacaftor/Tezacaftor/Ivacaftor in Children 6 Through 11 Years of Age with Cystic Fibrosis Heterozygous for F508del and a Minimal Function Mutation: A Phase 3b, Randomized, Placebo-controlled Study
- PMID: 35816621
- PMCID: PMC9746869
- DOI: 10.1164/rccm.202202-0392OC
Efficacy and Safety of Elexacaftor/Tezacaftor/Ivacaftor in Children 6 Through 11 Years of Age with Cystic Fibrosis Heterozygous for F508del and a Minimal Function Mutation: A Phase 3b, Randomized, Placebo-controlled Study
Abstract
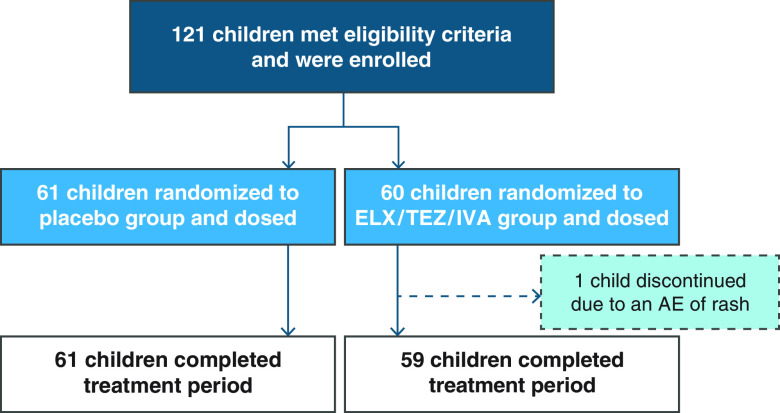
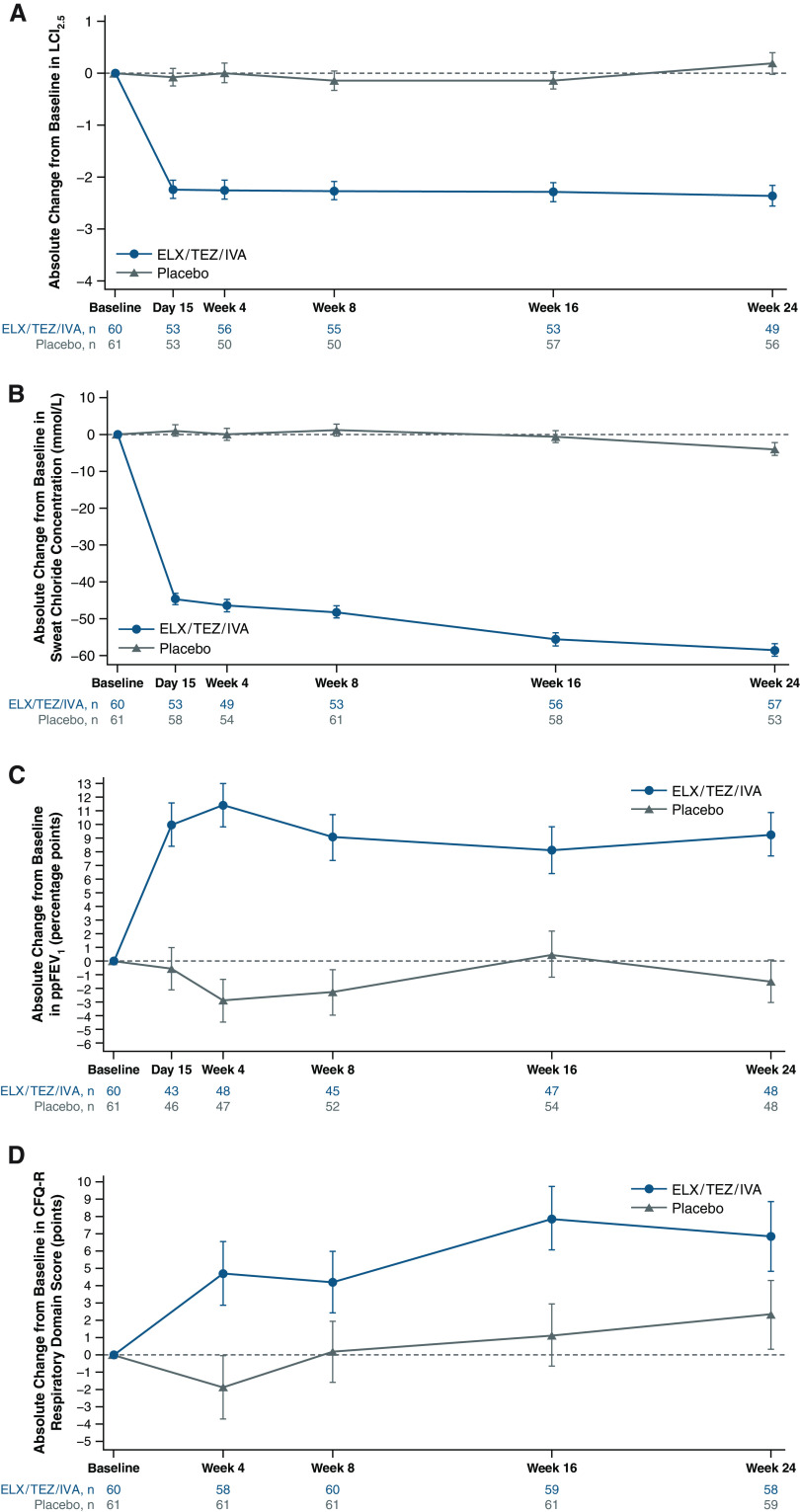
Rationale: The triple-combination regimen elexacaftor/tezacaftor/ivacaftor (ELX/TEZ/IVA) was shown to be safe and efficacious in children aged 6 through 11 years with cystic fibrosis and at least one F508del-CFTR allele in a phase 3, open-label, single-arm study. Objectives: To further evaluate the efficacy and safety of ELX/TEZ/IVA in children 6 through 11 years of age with cystic fibrosis heterozygous for F508del and a minimal function CFTR mutation (F/MF genotypes) in a randomized, double-blind, placebo-controlled phase 3b trial. Methods: Children were randomized to receive either ELX/TEZ/IVA (n = 60) or placebo (n = 61) during a 24-week treatment period. The dose of ELX/TEZ/IVA administered was based on weight at screening, with children <30 kg receiving ELX 100 mg once daily, TEZ 50 mg once daily, and IVA 75 mg every 12 hours, and children ⩾30 kg receiving ELX 200 mg once daily, TEZ 100 mg once daily, and IVA 150 mg every 12 hours (adult dose). Measurements and Main Results: The primary endpoint was absolute change in lung clearance index2.5 from baseline through Week 24. Children given ELX/TEZ/IVA had a mean decrease in lung clearance index2.5 of 2.29 units (95% confidence interval [CI], 1.97-2.60) compared with 0.02 units (95% CI, -0.29 to 0.34) in children given placebo (between-group treatment difference, -2.26 units; 95% CI, -2.71 to -1.81; P < 0.0001). ELX/TEZ/IVA treatment also led to improvements in the secondary endpoint of sweat chloride concentration (between-group treatment difference, -51.2 mmol/L; 95% CI, -55.3 to -47.1) and in the other endpoints of percent predicted FEV1 (between-group treatment difference, 11.0 percentage points; 95% CI, 6.9-15.1) and Cystic Fibrosis Questionnaire-Revised Respiratory domain score (between-group treatment difference, 5.5 points; 95% CI, 1.0-10.0) compared with placebo from baseline through Week 24. The most common adverse events in children receiving ELX/TEZ/IVA were headache and cough (30.0% and 23.3%, respectively); most adverse events were mild or moderate in severity. Conclusions: In this first randomized, controlled study of a cystic fibrosis transmembrane conductance regulator modulator conducted in children 6 through 11 years of age with F/MF genotypes, ELX/TEZ/IVA treatment led to significant improvements in lung function, as well as robust improvements in respiratory symptoms and cystic fibrosis transmembrane conductance regulator function. ELX/TEZ/IVA was generally safe and well tolerated in this pediatric population with no new safety findings.
Keywords: children; cystic fibrosis; elexacaftor; ivacaftor; tezacaftor.
Figures
Comment in
-
Evidence for Early Cystic Fibrosis Transmembrane Conductance Regulator Modulator Treatment for Children with Cystic Fibrosis Keeps Growing.Am J Respir Crit Care Med. 2022 Dec 1;206(11):1308-1310. doi: 10.1164/rccm.202208-1507ED. Am J Respir Crit Care Med. 2022. PMID: 35947636 Free PMC article. No abstract available.
References
-
- Riordan JR, Rommens JM, Kerem B, Alon N, Rozmahel R, Grzelczak Z, et al. Identification of the cystic fibrosis gene: cloning and characterization of complementary DNA. Science . 1989;245:1066–1073. - PubMed
-
- Cystic Fibrosis Mutation Database (CFTR1) 2011. http://www.genet.sickkids.on.ca/
-
- The Clinical and Functional TRanslation of CFTR (CFTR2) 2011. https://cftr2.org/
-
- Riordan JR. CFTR function and prospects for therapy. Annu Rev Biochem . 2008;77:701–726. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
