

Does [99mTc]-3,3-diphosphono-1,2-propanodicarboxylic acid (DPD) soft tissue uptake allow the identification of patients with the diagnosis of cardiac transthyretin-related (ATTR) amyloidosis with higher risk for polyneuropathy?
- PMID: 35817943
- PMCID: PMC9984356
- DOI: 10.1007/s12350-022-02986-7
Does [99mTc]-3,3-diphosphono-1,2-propanodicarboxylic acid (DPD) soft tissue uptake allow the identification of patients with the diagnosis of cardiac transthyretin-related (ATTR) amyloidosis with higher risk for polyneuropathy?
Abstract
Background: With the introduction of several drugs for the therapy of transthyretin-related amyloidosis (ATTR) which slow down the disease, early detection of polyneuropathy (PNP) is becoming increasingly of interest. [99mTc]-3,3-Diphosphono-1,2-Propanodicarboxylic Acid (DPD) bone scintigraphy, which is used for the diagnosis of cardiac (c)ATTR, can possibly make an important contribution in the identification of patients at risk for PNP.
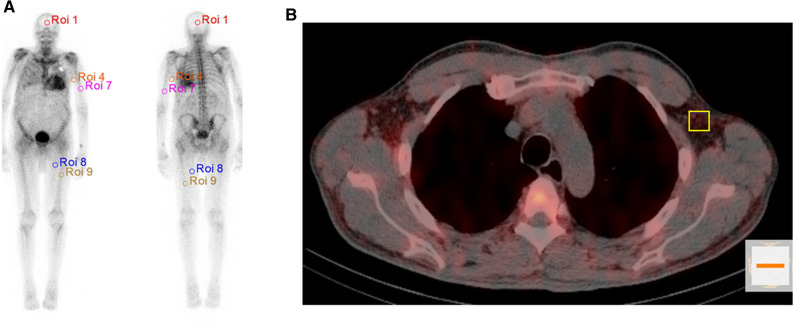
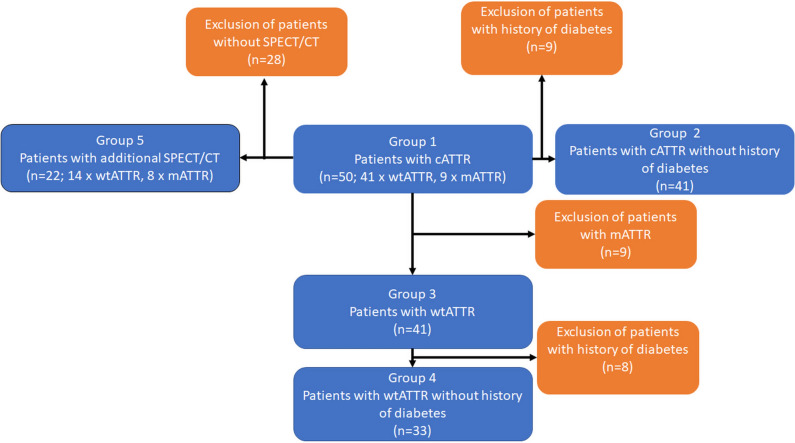
Methods: Fifty patients with cATTR, who underwent both planar whole-body DPD scintigraphy and nerve conduction studies (NCS) were retrospectively evaluated. A subgroup of 22 patients also underwent quantitative SPECT/CT of the thorax from which Standardized Uptake Values (SUVpeak) in the subcutaneous fat tissue of the left axillar region were evaluated.
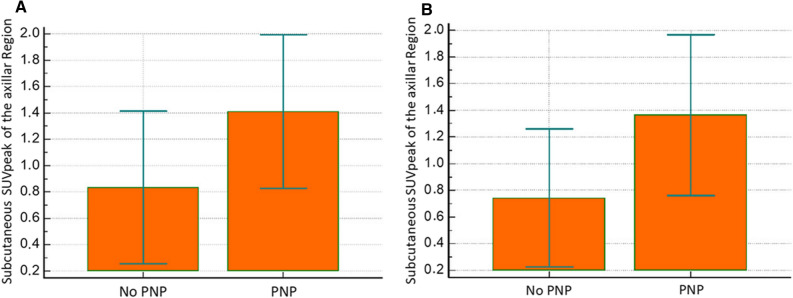
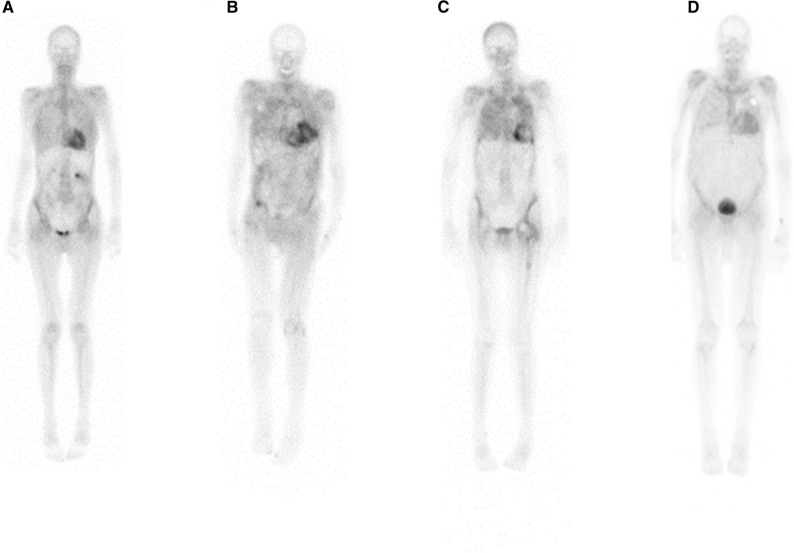
Results: The Perugini score was significantly increased in patients with cATTR and additional diagnosis of PNP compared to patients without (2.51 ± 0.51 vs 2.13 ± 0.52; P = 0.03). Quantitative SPECT/CT revealed that DPD uptake in the subcutaneous fat of the left axillar region was significantly increased in cATTR patients with compared to patients without (1.36 ± 0.60 vs 0.74 ± 0.52; P = 0.04).
Conclusion: This study suggests that DPD bone scintigraphy is a useful tool for identification of patients with cATTR and a risk for PNP due to increased DPD soft tissue uptake.
Keywords: ATTR; Amyloidosis; Bone scintigraphy; Polyneuropathy.
© 2022. The Author(s).
Figures
Comment in
-
Bone scintigraphy imaging and transthyretin-related (ATTR) cardiac amyloidosis: New tricks from an old tool?J Nucl Cardiol. 2023 Feb;30(1):368-370. doi: 10.1007/s12350-022-03032-2. Epub 2022 Jul 22. J Nucl Cardiol. 2023. PMID: 35869405 Free PMC article. No abstract available.
-
Correlation between DPD soft tissue uptake and polyneuropathy in ATTR amyloidosis.J Nucl Cardiol. 2023 Apr;30(2):858. doi: 10.1007/s12350-023-03217-3. Epub 2023 Feb 10. J Nucl Cardiol. 2023. PMID: 36764985 No abstract available.
References
-
- Lachmann HJ, Hawkins PN. Systemic amyloidosis. Cardiavascular Ren. 2006;6:214–220. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
