

Metagenomic prediction of antimicrobial resistance in critically ill patients with lower respiratory tract infections
- PMID: 35818068
- PMCID: PMC9275031
- DOI: 10.1186/s13073-022-01072-4
Metagenomic prediction of antimicrobial resistance in critically ill patients with lower respiratory tract infections
Abstract
Background: Antimicrobial resistance (AMR) is rising at an alarming rate and complicating the management of infectious diseases including lower respiratory tract infections (LRTI). Metagenomic next-generation sequencing (mNGS) is a recently established method for culture-independent LRTI diagnosis, but its utility for predicting AMR has remained unclear. We aimed to assess the performance of mNGS for AMR prediction in bacterial LRTI and demonstrate proof of concept for epidemiological AMR surveillance and rapid AMR gene detection using Cas9 enrichment and nanopore sequencing.
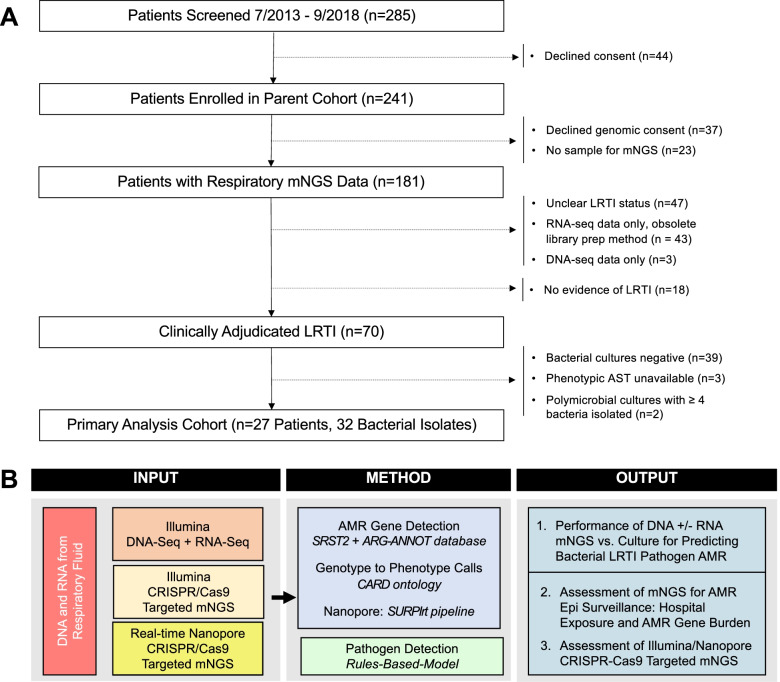
Methods: We studied 88 patients with acute respiratory failure between 07/2013 and 9/2018, enrolled through a previous observational study of LRTI. Inclusion criteria were age ≥ 18, need for mechanical ventilation, and respiratory specimen collection within 72 h of intubation. Exclusion criteria were decline of study participation, unclear LRTI status, or no matched RNA and DNA mNGS data from a respiratory specimen. Patients with LRTI were identified by clinical adjudication. mNGS was performed on lower respiratory tract specimens. The primary outcome was mNGS performance for predicting phenotypic antimicrobial susceptibility and was assessed in patients with LRTI from culture-confirmed bacterial pathogens with clinical antimicrobial susceptibility testing (n = 27 patients, n = 32 pathogens). Secondary outcomes included the association between hospital exposure and AMR gene burden in the respiratory microbiome (n = 88 patients), and AMR gene detection using Cas9 targeted enrichment and nanopore sequencing (n = 10 patients).
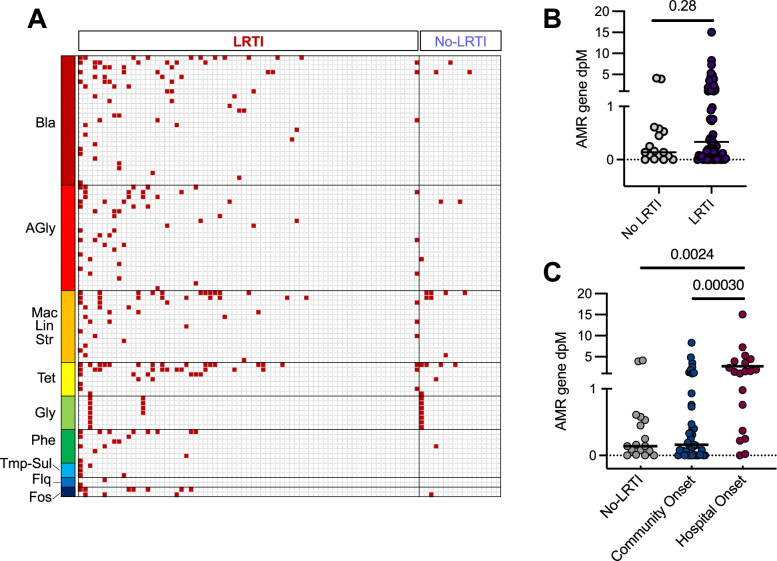
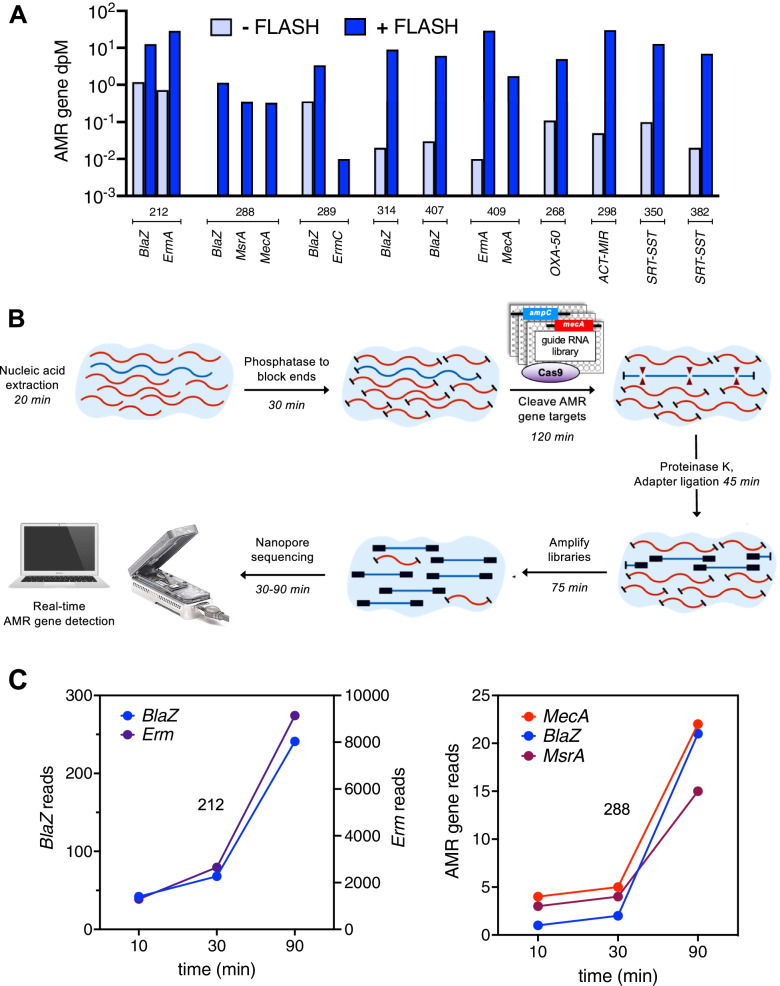
Results: Compared to clinical antimicrobial susceptibility testing, the performance of respiratory mNGS for predicting AMR varied by pathogen, antimicrobial, and nucleic acid type sequenced. For gram-positive bacteria, a combination of RNA + DNA mNGS achieved a sensitivity of 70% (95% confidence interval (CI) 47-87%) and specificity of 95% (CI 85-99%). For gram-negative bacteria, sensitivity was 100% (CI 87-100%) and specificity 64% (CI 48-78%). Patients with hospital-onset LRTI had a greater AMR gene burden in their respiratory microbiome versus those with community-onset LRTI (p = 0.00030), or those without LRTI (p = 0.0024). We found that Cas9 targeted sequencing could enrich for low abundance AMR genes by > 2500-fold and enabled their rapid detection using a nanopore platform.
Conclusions: mNGS has utility for the detection and surveillance of resistant bacterial LRTI pathogens.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- O’Neill J. Tackling drug-resistant infections globally: final report and recommendations. London, UK May 16, 2016 2016. 2016; published online May 16. http://amr-review.org/Publications.
-
- van der Eerden MM, Vlaspolder F, de Graaff CS, et al. Comparison between pathogen directed antibiotic treatment and empirical broad spectrum antibiotic treatment in patients with community acquired pneumonia: a prospective randomised study. Thorax. 2005;60:672–678. doi: 10.1136/thx.2004.030411. - DOI - PMC - PubMed
