

A 73-Year-Old Woman Treated for Rheumatoid Arthritis with Lower Rectal Carcinoma Who Underwent Abdominoperineal Resection, Lateral Regional Lymph Node Resection, and Partial Hepatectomy by Hand-Assisted Laparoscopic Surgery (HALS): A Case Report
- PMID: 35818321
- PMCID: PMC9288853
- DOI: 10.12659/AJCR.936106
A 73-Year-Old Woman Treated for Rheumatoid Arthritis with Lower Rectal Carcinoma Who Underwent Abdominoperineal Resection, Lateral Regional Lymph Node Resection, and Partial Hepatectomy by Hand-Assisted Laparoscopic Surgery (HALS): A Case Report
Abstract
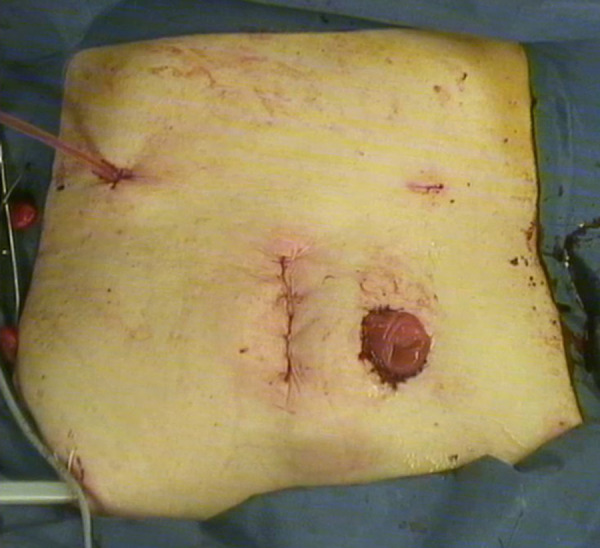
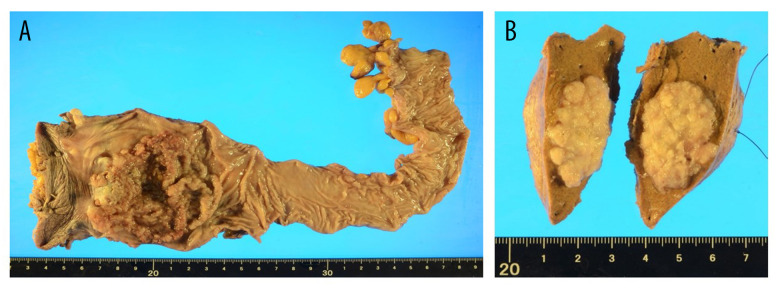
BACKGROUND This report describes the case of a 73-year-old woman treated for rheumatoid arthritis with lower rectal carcinoma who underwent abdominoperineal resection, lateral regional lymph node resection, and partial hepatectomy by hand-assisted laparoscopic surgery (HALS). More recently, HALS has proven to be useful in multiple organ resections. CASE REPORT A 73-year-old woman who presented with hematochezia was diagnosed with lower rectal cancer and referred to our hospital. The patient had a history of rheumatoid arthritis and was taking oral nonsteroidal anti-inflammatory drugs. After further evaluation, the patient was diagnosed with stage IV rectal cancer with a metastatic liver lesion and a right lateral lymph node metastasis. All lesions were resected using HALS. A 50-mm longitudinal umbilical incision was created for use as a hand access site, and 3 ports with a diameter of 5 mm each were inserted into the lower abdomen to perform right lateral lymph node dissection and abdominoperineal resection. HALS was performed in the upper abdomen, where the liver was used to partially resect segment S6. The patient was discharged without complications 13 days after the operation. CONCLUSIONS In this complex case of advanced rectal carcinoma with liver metastases, use of the HALS surgical method was shown to be possible. Immunomodulatory treatment for rheumatoid arthritis may have influenced the outcome for this patient.
Conflict of interest statement
Figures




Similar articles
-
Laparoscopic abdominoperineal resection with lateral lymph node dissection for advanced rectal and prostate cancer with synchronous lateral lymph node metastases.Asian J Endosc Surg. 2019 Jan;12(1):118-121. doi: 10.1111/ases.12598. Epub 2018 May 10. Asian J Endosc Surg. 2019. PMID: 29745478
-
[Laparoscopic Lateral Lymph Node Dissection for Rectal Cancer with Lateral Lymph Node Metastasis - A Case Report].Gan To Kagaku Ryoho. 2016 Nov;43(12):2292-2294. Gan To Kagaku Ryoho. 2016. PMID: 28133299 Japanese.
-
[Transanal lateral lymph node dissection surgery for 5 cases of mid-low rectal cancer].Zhonghua Wei Chang Wai Ke Za Zhi. 2019 Aug 25;22(8):781-785. doi: 10.3760/cma.j.issn.1671-0274.2019.08.014. Zhonghua Wei Chang Wai Ke Za Zhi. 2019. PMID: 31422618 Chinese.
-
[A Case of Isolated Lateral Pelvic Lymph Node Recurrence after TME for Early Lower Rectal Cancer Treated with Laparoscopic Lateral Lymph Node Dissection].Gan To Kagaku Ryoho. 2018 Apr;45(4):734-736. Gan To Kagaku Ryoho. 2018. PMID: 29650851 Review. Japanese.
-
Laparoscopic abdominoperineal resection for anorectal cancer.Am Surg. 1998 Jan;64(1):12-8. Am Surg. 1998. PMID: 9457031 Review.
References
-
- Mukai M, Kishima K, Tajima T, et al. Efficacy of hybrid 2-port hand-assisted laparoscopic surgery (Mukai’s operation) in patients with colorectal cancer. Oncol Rep. 2009;22:893–99. - PubMed
-
- Mukai M. Nankodo Co., Ltd; Tokyo [in Japanese]: 2014. [Base techniques of HALS for colorectal cancer. HALS (hand-assisted laparoscopic surgery).] pp. 19–41.
-
- Mukai M, Yokoyama D, Uda S, et al. [Hand-assisted laparoscopic surgery (HALS) for lower rectal cancer.] Surgery. 2016;78:944–49. [in Japanese]
-
- Tajima T, Mukai M, Koike T, et al. Better survival after hand-assisted laparoscopic surgery than conventional laparotomy for rectal cancer: Five year results from a single center in Japan. Clin in Surg. 2017;2:1368.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
