

Topical Losartan and Corticosteroid Additively Inhibit Corneal Stromal Myofibroblast Generation and Scarring Fibrosis After Alkali Burn Injury
- PMID: 35819289
- PMCID: PMC9287619
- DOI: 10.1167/tvst.11.7.9
Topical Losartan and Corticosteroid Additively Inhibit Corneal Stromal Myofibroblast Generation and Scarring Fibrosis After Alkali Burn Injury
Erratum in
-
Erratum in: Topical Losartan and Corticosteroid Additively Inhibit Corneal Stromal Myofibroblast Generation and Scarring Fibrosis After Alkali Burn Injury.Transl Vis Sci Technol. 2022 Oct 3;11(10):30. doi: 10.1167/tvst.11.10.30. Transl Vis Sci Technol. 2022. PMID: 36259680 Free PMC article. No abstract available.
Abstract
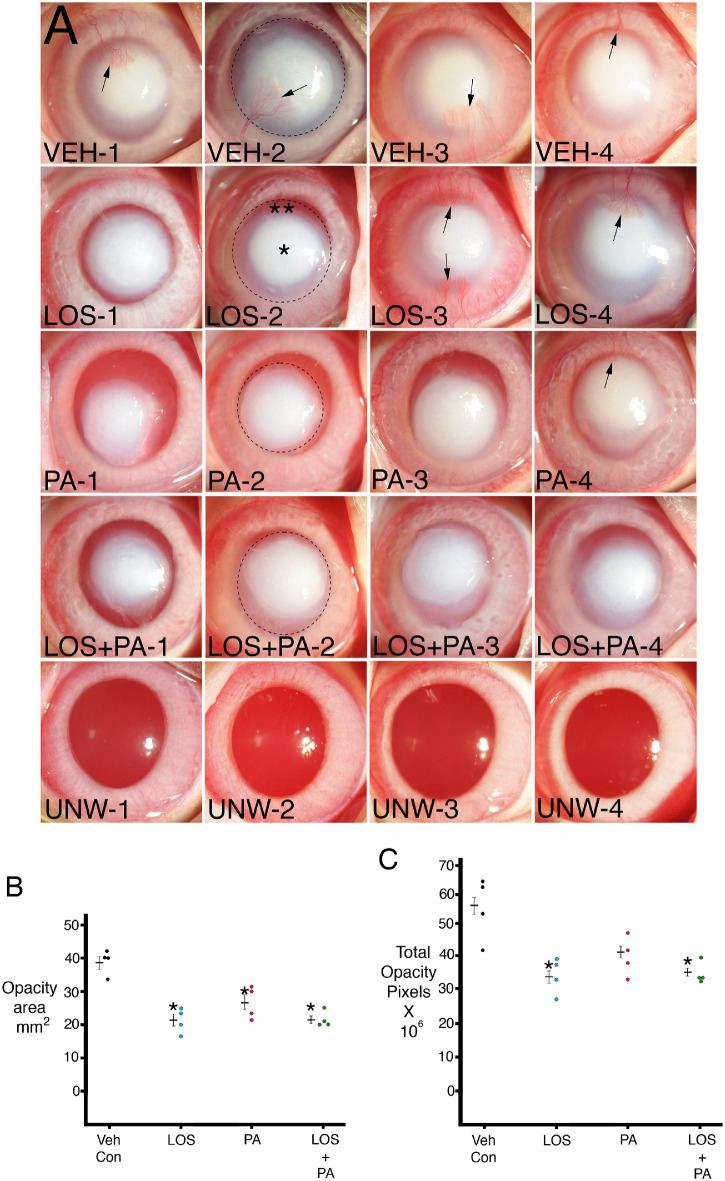
Purpose: To evaluate the efficacy of losartan and prednisolone acetate in inhibiting corneal scarring fibrosis after alkali burn injury in rabbits.
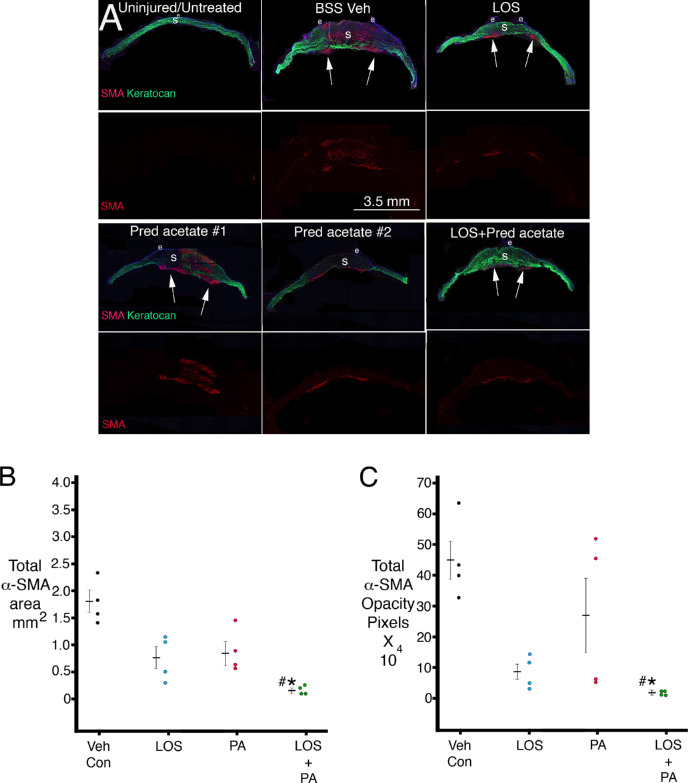
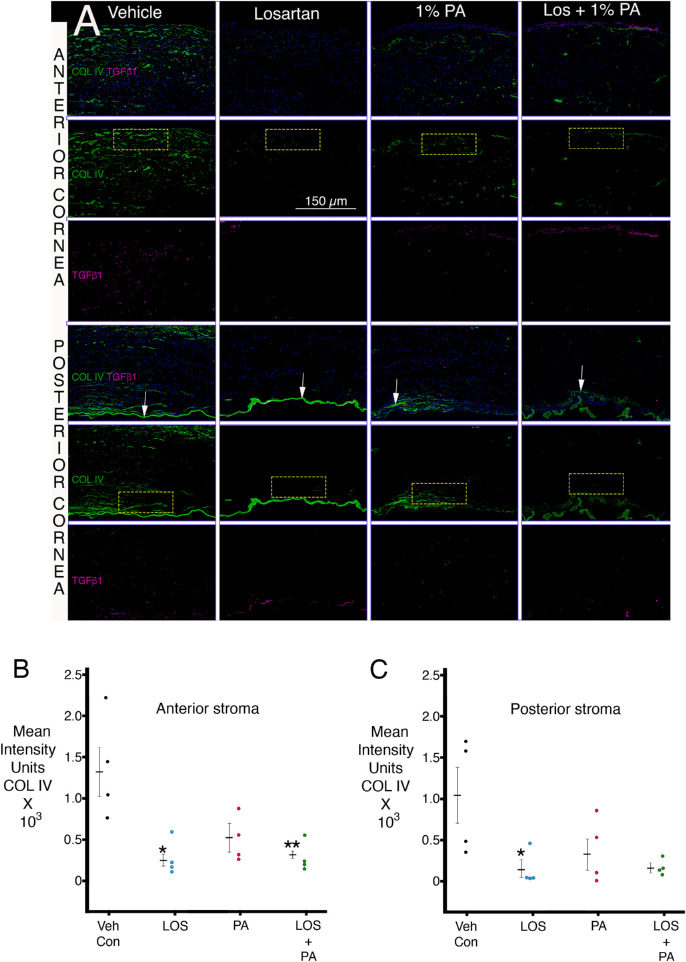
Methods: Sixteen New Zealand White rabbits were included. Alkali injuries were produced using 1N sodium hydroxide on a 5-mm diameter Whatman #1 filter paper for 1 minute. Four corneas in each group were treated six times per day for 1 month with 50 µL of (1) 0.8 mg/mL losartan in balanced salt solution (BSS), (2) 1% prednisolone acetate, (3) combined 0.8 mg/mL losartan and 1% prednisolone acetate, or (4) BSS. Area of opacity and total opacity were analyzed in standardized slit-lamp photos with ImageJ. Corneas in both groups were cryofixed in Optimal cutting temperature (OCT) compound at 1 month after surgery, and immunohistochemistry was performed for alpha-smooth muscle actin (α-SMA) and keratocan or transforming growth factor β1 and collagen type IV with ImageJ quantitation.
Results: Combined topical losartan and prednisolone acetate significantly decreased slit-lamp opacity area and intensity, as well as decreased stromal myofibroblast α-SMA area and intensity of staining per section and confined myofibroblasts to only the posterior stroma with repopulation of the anterior and mid-stroma with keratocan-positive keratocytes after 1 month of treatment. Corneal fibroblasts produced collagen type IV not associated with basement membranes, and this production was decreased by topical losartan.
Conclusions: Combined topical losartan and prednisolone acetate decreased myofibroblast-associated fibrosis after corneal alkali burns that produced full-thickness injury, including corneal endothelial damage. Increased dosages and duration of treatment may further decrease scarring fibrosis.
Translational relevance: Topical losartan and prednisolone acetate decrease myofibroblast-mediated scarring fibrosis after corneal injury.
Conflict of interest statement
Disclosure:
Figures
References
-
- Jester JV, Huang J, Petroll WM, Cavanagh HD.. TGFbeta induced myofibroblast differentiation of rabbit keratocytes requires synergistic TGFbeta, PDGF and integrin signaling . Exp Eye Res. 2002; 75: 645–657. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
