

Variation in Clinical Characteristics and Longitudinal Outcomes in Individuals with Opioid Use Disorder Diagnosis Codes
- PMID: 35819683
- PMCID: PMC9971398
- DOI: 10.1007/s11606-022-07732-w
Variation in Clinical Characteristics and Longitudinal Outcomes in Individuals with Opioid Use Disorder Diagnosis Codes
Abstract
Background: Patterns of opioid use vary, including prescribed use without aberrancy, limited aberrant use, and potential opioid use disorder (OUD). In clinical practice, similar opioid-related International Classification of Disease (ICD) codes are applied across this spectrum, limiting understanding of how groups vary by sociodemographic factors, comorbidities, and long-term risks.
Objective: (1) Examine how Veterans assigned opioid abuse/dependence ICD codes vary at diagnosis and with respect to long-term risks. (2) Determine whether those with limited aberrant use share more similarities to likely OUD vs those using opioids as prescribed.
Design: Longitudinal observational cohort study.
Participants: National sample of Veterans categorized as having (1) likely OUD, (2) limited aberrant opioid use, or (3) prescribed, non-aberrant use based upon enhanced medical chart review.
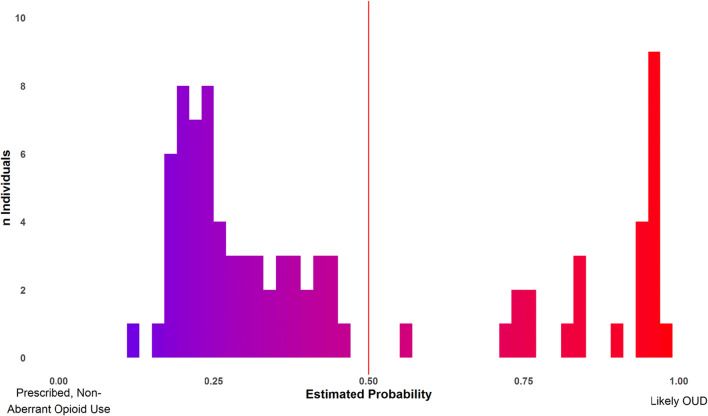
Main measures: Comparison of sociodemographic and clinical factors at diagnosis and rates of age-adjusted mortality, non-fatal opioid overdose, and hospitalization after diagnosis. An exploratory machine learning analysis investigated how closely those with limited aberrant use resembled those with likely OUD.
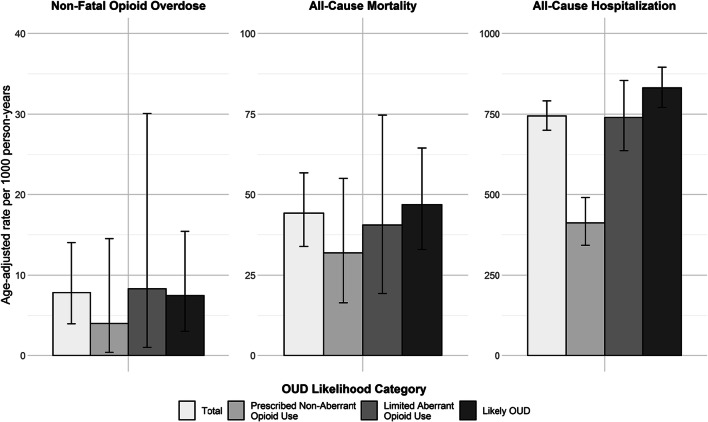
Key results: Veterans (n = 483) were categorized as likely OUD (62.1%), limited aberrant use (17.8%), and prescribed, non-aberrant use (20.1%). Age, proportion experiencing homelessness, chronic pain, anxiety disorders, and non-opioid substance use disorders differed by group. All-cause mortality was high (44.2 per 1000 person-years (95% CI 33.9, 56.7)). Hospitalization rates per 1000 person-years were highest in the likely OUD group (831.5 (95% CI 771.0, 895.5)), compared to limited aberrant use (739.8 (95% CI 637.1, 854.4)) and prescribed, non-aberrant use (411.9 (95% CI 342.6, 490.4). The exploratory analysis reclassified 29.1% of those with limited aberrant use as having likely OUD with high confidence.
Conclusions: Veterans assigned opioid abuse/dependence ICD codes are heterogeneous and face variable long-term risks. Limited aberrant use confers increased risk compared to no aberrant use, and some may already have OUD. Findings warrant future investigation of this understudied population.
Keywords: chronic pain; long-term opioid therapy; opioid use disorder; risk.
© 2022. This is a U.S. Government work and not under copyright protection in the US; foreign copyright protection may apply.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Identifying patients with opioid use disorder using International Classification of Diseases (ICD) codes: Challenges and opportunities.Addiction. 2024 Jan;119(1):160-168. doi: 10.1111/add.16338. Epub 2023 Sep 15. Addiction. 2024. PMID: 37715369 Free PMC article.
-
How Is Preoperative Opioid Use Associated With Readmissions and Outcomes in Lower Extremity Trauma?Clin Orthop Relat Res. 2025 May 1;483(5):918-927. doi: 10.1097/CORR.0000000000003346. Epub 2024 Dec 20. Clin Orthop Relat Res. 2025. PMID: 39787379
-
Cannabis Legalization and Opioid Use Disorder in Veterans Health Administration Patients.JAMA Health Forum. 2025 Jun 7;6(6):e251369. doi: 10.1001/jamahealthforum.2025.1369. JAMA Health Forum. 2025. PMID: 40512510 Free PMC article.
-
Supervised dosing with a long-acting opioid medication in the management of opioid dependence.Cochrane Database Syst Rev. 2017 Apr 27;4(4):CD011983. doi: 10.1002/14651858.CD011983.pub2. Cochrane Database Syst Rev. 2017. PMID: 28447766 Free PMC article.
-
Prevalence of problematic pharmaceutical opioid use in patients with chronic non-cancer pain: A systematic review and meta-analysis.Addiction. 2024 Nov;119(11):1904-1922. doi: 10.1111/add.16616. Epub 2024 Aug 7. Addiction. 2024. PMID: 39111346
Cited by
-
SubgroupTE: Advancing Treatment Effect Estimation with Subgroup Identification.ACM Trans Intell Syst Technol. 2025 Jun;16(3):71. doi: 10.1145/3718097. Epub 2025 Jun 10. ACM Trans Intell Syst Technol. 2025. PMID: 40575765 Free PMC article.
-
Heterogeneous Treatment Effect Estimation with Subpopulation Identification for Personalized Medicine in Opioid Use Disorder.Proc IEEE Int Conf Data Min. 2023 Dec;2023:1079-1084. doi: 10.1109/icdm58522.2023.00127. Epub 2024 Feb 5. Proc IEEE Int Conf Data Min. 2023. PMID: 38389702 Free PMC article.
-
Perioperative opioid prescribing and iatrogenic opioid use disorder and overdose: a state-of-the-art narrative review.Reg Anesth Pain Med. 2024 Aug 5;49(8):602-608. doi: 10.1136/rapm-2023-104944. Reg Anesth Pain Med. 2024. PMID: 37931982 Free PMC article. Review.
References
-
- Substance Abuse and Mental Health Services Administration. Key substance use and mental health indicators in the United States: results from the 2018 National Survey on Drug Use and Health. HHS Publ No PEP19-5068, NSDUH Ser H-54. 2019;170:51-58. https://www.samhsa.gov/data/
-
- Substance-related and addictive disorders. In: Diagnostic and Statistical Manual of Mental Disorders. 5th ed. American Psychiatric Association; 2013. 10.1176/appi.books.9780890425596.dsm16.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
