

Ergogenic value of oxygen supplementation in chronic obstructive pulmonary disease
- PMID: 35819698
- PMCID: PMC9352614
- DOI: 10.1007/s11739-022-03037-2
Ergogenic value of oxygen supplementation in chronic obstructive pulmonary disease
Abstract
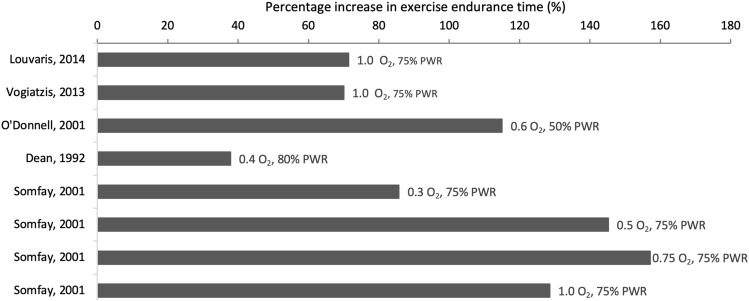
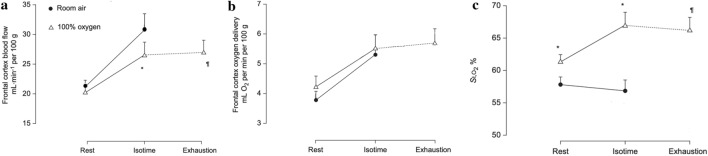
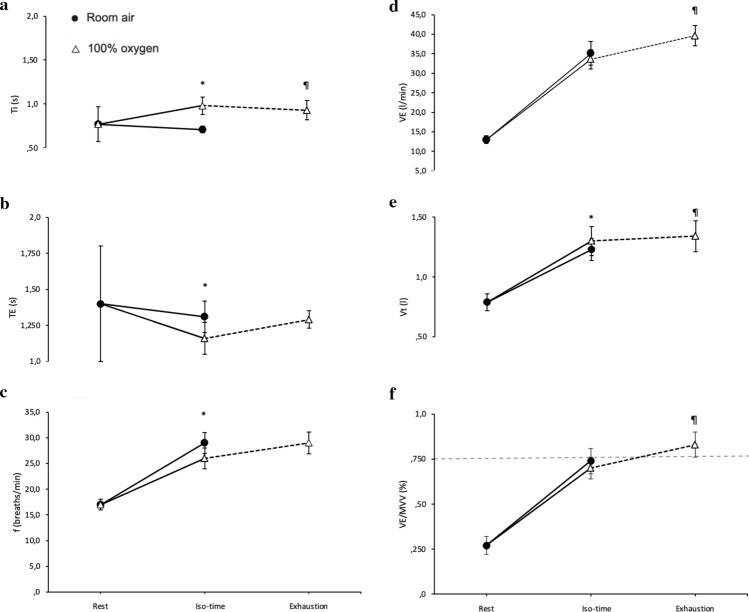
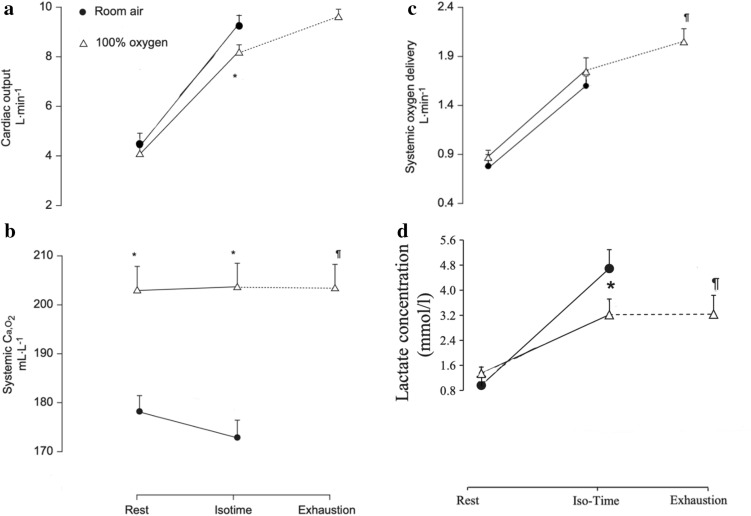
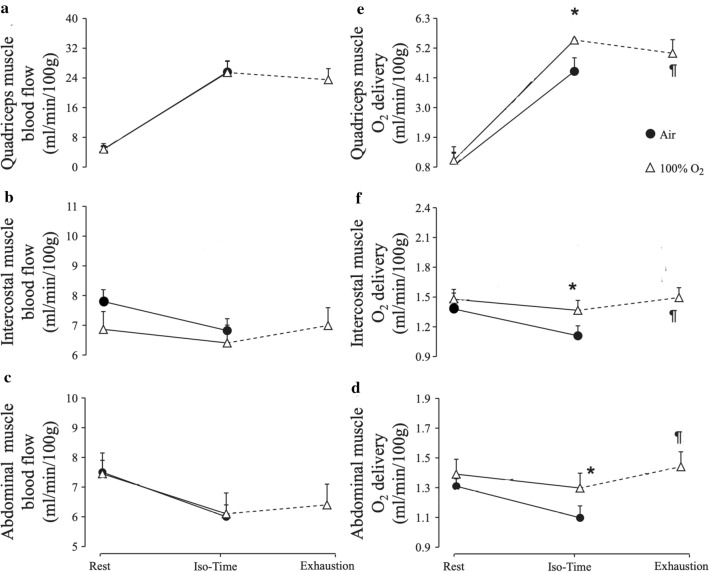
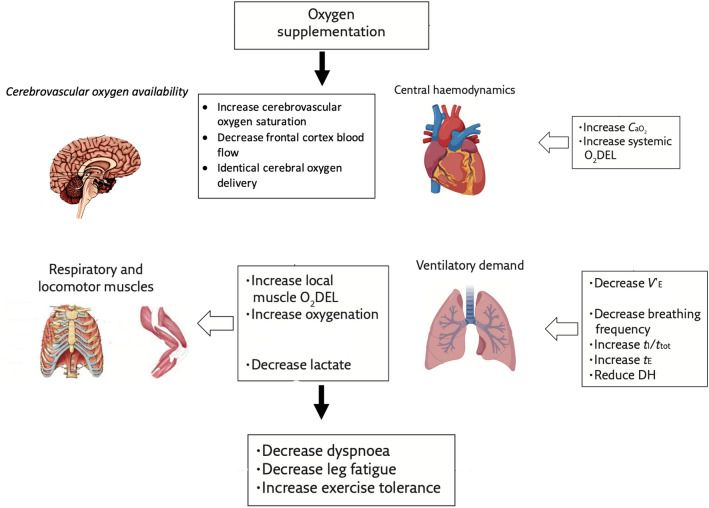
Patients with COPD exhibit limited exercise endurance time compared to healthy age-matched individuals. Oxygen supplementation is often applied to improve endurance time during pulmonary rehabilitation in patients with COPD and thus a comprehensive understanding of the mechanisms leading to improved endurance is desirable. This review analyses data from two studies by our research group investigating the effect of oxygen supplementation on cerebrovascular, systemic, respiratory and locomotor muscle oxygen availability on the same cohort of individuals with advanced COPD, and the mechanisms associated with improved endurance time in hyperoxia, which was essentially doubled (at the same power output). In hyperoxia at isotime (the time at which patients became exhausted in normoxia) exercise was associated with greater respiratory and locomotor muscle (but not frontal cortex) oxygen delivery (despite lower cardiac output), lower lactate concentration and less tachypnoea. Frontal cortex oxygen saturation was higher, and respiratory drive lower. Hence, improved endurance in hyperoxia appears to be facilitated by several factors: increased oxygen availability to the respiratory and locomotor muscles, less metabolic acidosis, and lower respiratory drive. At exhaustion in both normoxia and hyperoxia, only cardiac output and breathing pattern were not different between conditions. However, minute ventilation in hyperoxia exceeded the critical level of ventilatory constraints (VE/MVV > 75-80%). Lactate remained lower and respiratory and locomotor muscle oxygen delivery greater in hyperoxia, suggesting greater muscle oxygen availability improving muscle function. Taken together, these findings suggest that central haemodynamic and ventilatory limitations and not contracting muscle conditions dictate endurance time in COPD during exercise in hyperoxia.
Keywords: COPD; Exercise tolerance; Oxygen supplementation.
© 2022. The Author(s).
Figures
Similar articles
-
Greater exercise tolerance in COPD during acute interval, compared to equivalent constant-load, cycle exercise: physiological mechanisms.J Physiol. 2020 Sep;598(17):3613-3629. doi: 10.1113/JP279531. Epub 2020 Jun 16. J Physiol. 2020. PMID: 32472698
-
Exercise tolerance with helium-hyperoxia versus hyperoxia in hypoxaemic patients with COPD.Eur Respir J. 2013 Aug;42(2):362-70. doi: 10.1183/09031936.00087812. Epub 2012 Nov 22. Eur Respir J. 2013. PMID: 23180584 Clinical Trial.
-
Effects of oxygen supplementation on cerebral oxygenation during exercise in chronic obstructive pulmonary disease patients not entitled to long-term oxygen therapy.Clin Physiol Funct Imaging. 2012 Jan;32(1):52-8. doi: 10.1111/j.1475-097X.2011.01054.x. Epub 2011 Oct 3. Clin Physiol Funct Imaging. 2012. PMID: 22152079 Clinical Trial.
-
The Effects of Hyperoxia on Sea-Level Exercise Performance, Training, and Recovery: A Meta-Analysis.Sports Med. 2018 Jan;48(1):153-175. doi: 10.1007/s40279-017-0791-2. Sports Med. 2018. PMID: 28975517 Review.
-
Enhancement of exercise performance in COPD patients by hyperoxia: a call for research.Chest. 2002 Nov;122(5):1830-6. doi: 10.1378/chest.122.5.1830. Chest. 2002. PMID: 12426288 Review.
Cited by
-
Hyperoxia improves exercise capacity in cardiopulmonary disease: a series of randomised controlled trials.ERJ Open Res. 2023 Mar 27;9(2):00563-2022. doi: 10.1183/23120541.00563-2022. eCollection 2023 Mar. ERJ Open Res. 2023. PMID: 37009023 Free PMC article.
-
Pulmonary rehabilitation and physical interventions.Eur Respir Rev. 2023 Jun 7;32(168):220222. doi: 10.1183/16000617.0222-2022. Print 2023 Jun 30. Eur Respir Rev. 2023. PMID: 37286219 Free PMC article. Review.
-
Respiratory and locomotor muscle blood flow measurements using near-infrared spectroscopy and indocyanine green dye in health and disease.Chron Respir Dis. 2024 Jan-Dec;21:14799731241246802. doi: 10.1177/14799731241246802. Chron Respir Dis. 2024. PMID: 38590151 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
