

A direct comparison of patient-reported outcomes and experiences in alternative models of maternity care in Queensland, Australia
- PMID: 35819947
- PMCID: PMC9275696
- DOI: 10.1371/journal.pone.0271105
A direct comparison of patient-reported outcomes and experiences in alternative models of maternity care in Queensland, Australia
Abstract
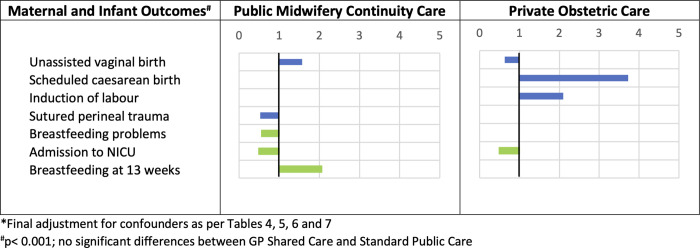
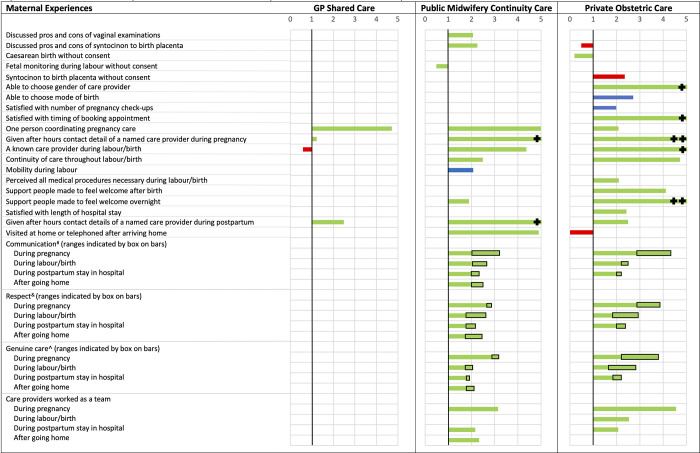
We aimed to directly compare women's pregnancy to postpartum outcomes and experiences across the major maternity models of care offered in Queensland, Australia. We conducted secondary analyses of self-reported data collected in 2012 from a state-wide sample of women who had recently given birth in Queensland (response rate = 30.4%). Logistic regression was used to estimate the odds of outcomes and experiences associated with three models (GP Shared Care, Public Midwifery Continuity Care, Private Obstetric Care) compared with Standard Public Care, adjusting for relevant maternal characteristics and clinical covariates. Of 2,802 women, 18.2% received Standard Public Care, 21.7% received GP Shared Care, 12.9% received Public Midwifery Continuity Care, and 47.1% received Private Obstetric Care. There were minimal differences for women in GP Shared Care. Women in Public Midwifery Continuity Care were less likely to have a scheduled caesarean and more likely to have an unassisted vaginal birth, experience freedom of mobility during labour and informed consent processes for inducing labour, vaginal examinations, fetal monitoring and receiving Syntocinon to birth their placenta, and report highest quality interpersonal care. They had fewer vaginal examinations, lower odds of perineal trauma requiring sutures and anxiety after birth, shorter postpartum hospital stays, and higher odds of a home postpartum care visit. Women in Private Obstetric Care were more likely to have their labour induced, a scheduled caesarean birth, experience informed consent processes for caesarean, and report highest quality interpersonal care, but less likely to experience unassisted vaginal birth and informed consent for Syntocinon to birth their placenta. There is an urgent need to communicate variations between maternity models across the range of outcome and experiential measures that are important to women; build more rigorous comparative evidence for Private Midwifery Care; and prioritise experiential and out-of-pocket cost comparisons in further research to enable woman-centred informed decision-making.
Conflict of interest statement
We have read the journal’s policy and the authors of this manuscript have the following competing interests: YM has previously received funding for the development of patient decision aids, including resources for women to choose between models of maternity care, and for establishing a state-wide survey of recent maternity consumers’ experience of maternity care across different models of care in Queensland, Australia. The funding bodies for that work had no involvement in the research reported here. EM is employed by a health service at which some participants in this study gave birth. EM was not employed by the health service at the time of data collection (2012) and the health service had no involvement or influence in the analysis of the data for the work reported in this manuscript. JT and ST have no competing interests to declare. This does not alter our adherence to PLOS ONE policies on sharing data and materials
Figures
References
-
- Doherty D, Hornbuckle J, Hutchinson M, Henderson J, Montague G, Newnham J. Evaluation of pregnancy outcomes and cost-effectiveness of models of antenatal care and preferred setting for labour and birth care in women at low risk of pregnancy complications. Perth: Department of Health, Western Australia; 2008.
-
- Wilson KL, Sirois FM. Birth attendant choice and satisfaction with antenatal care: The role of birth philosophy, relational style, and health self-efficacy. J Reprod Infant Psychol. 2010;28(1):69–83. doi: 10.1080/02646830903190946 - DOI
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
