

Time to recovery and its predictors among critically ill patients on mechanical ventilation from intensive care unit in Ethiopia: a retrospective follow up study
- PMID: 35820844
- PMCID: PMC9277794
- DOI: 10.1186/s12873-022-00689-3
Time to recovery and its predictors among critically ill patients on mechanical ventilation from intensive care unit in Ethiopia: a retrospective follow up study
Abstract
Introduction: For critically ill patients, mechanical ventilation is considered a pillar of respiratory life support. The mortality of victims in intensive care units is high in resource-constrained Sub-Saharan African countries. The recovery and prognosis of mechanically ventilated victims are unknown, according to evidence. The goal of the study was to see how long critically ill patients on mechanical ventilation survived.
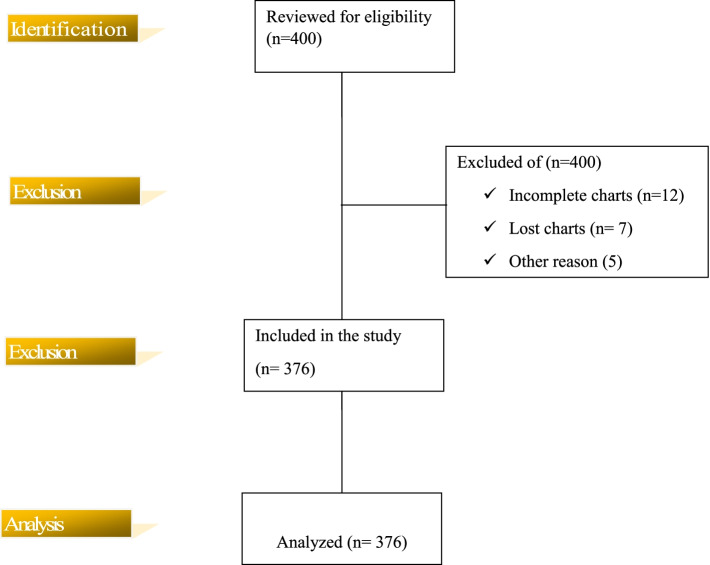
Methods: A retrospective follow-up study was conducted. A total of 376 study medical charts were reviewed. Data was collected through reviewing medical charts. Data was entered into Epi-data manager version 4.6.0.4 and analyzed through Stata version 16. Descriptive analysis was performed. Kaplan- Meier survival estimates and log rank tests were performed. Cox proportional hazard model was undertaken.
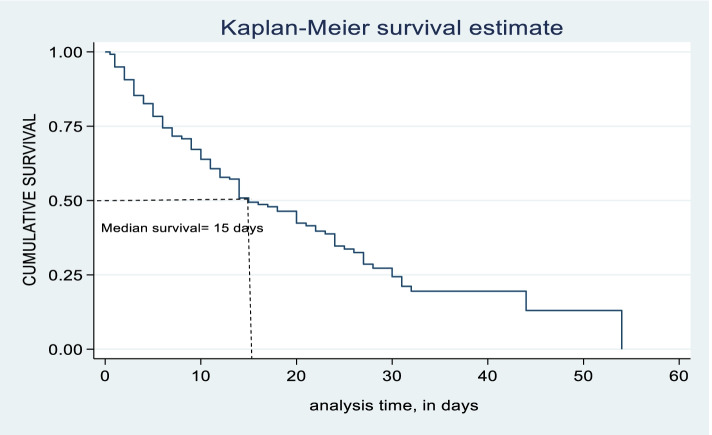
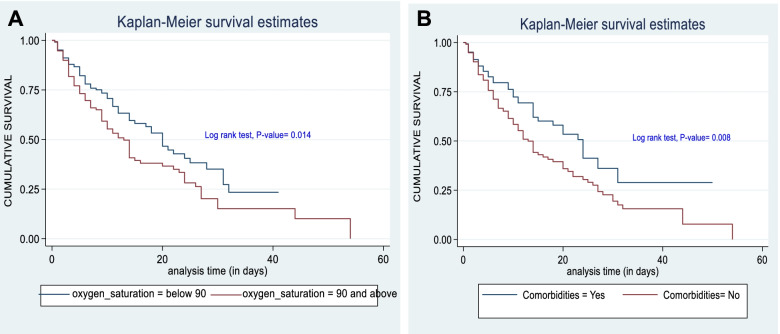
Results: Median recovery time was 15 days (IQR: 6-30) with a total recovery rate of 4.49 per 100 person-days. In cox proportional hazard regression, diagnosis category {AHR: 1.690, 95% CI: (1.150- 2.485)}, oxygen saturation {AHR: 1.600, 95% CI: (1.157- 2.211)}, presence of comorbidities {AHR: 1.774, 95% CI: (1.250-2.519)}, Glasgow coma scale {AHR: 2.451, 95% CI: (1.483- 4.051)}, and use of tracheostomy {AHR: 0.276, 95% CI: (0.180-0.422)} were statistically significant predictors.
Discussion: Based on the outcomes of this study, discussions with suggested possible reasons and its implications were provided.
Conclusion and recommendations: Duration and recovery rate of patients on mechanical ventilation is less than expected of world health organization standard. Diagnosis category, oxygen saturation, comorbidities, Glasgow coma scale and use of tracheostomy were statistically significant predictors. Mechanical ventilation durations should be adjusted for chronic comorbidities, trauma, and use of tracheostomy.
Keywords: Artificial respiration; Intensive care unit; Mechanical ventilation; Predictor; Recovery; Time.
© 2022. The Author(s).
Conflict of interest statement
The authors declared that there was no conflict of interest.
Figures
References
-
- Yang, L., et al., Home mechanical ventilation: A retrospective review of safety incidents using the World Health Organization International Patient Safety Event classification. Canadian journal of respiratory therapy: CJRT= Revue canadienne de la therapie respiratoire: RCTR, 2016. 52(3): p. 85. - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
