

School-based mindfulness training in early adolescence: what works, for whom and how in the MYRIAD trial?
- PMID: 35820993
- PMCID: PMC9340034
- DOI: 10.1136/ebmental-2022-300439
School-based mindfulness training in early adolescence: what works, for whom and how in the MYRIAD trial?
Abstract
Background: Preventing mental health problems in early adolescence is a priority. School-based mindfulness training (SBMT) is an approach with mixed evidence.
Objectives: To explore for whom SBMT does/does not work and what influences outcomes.
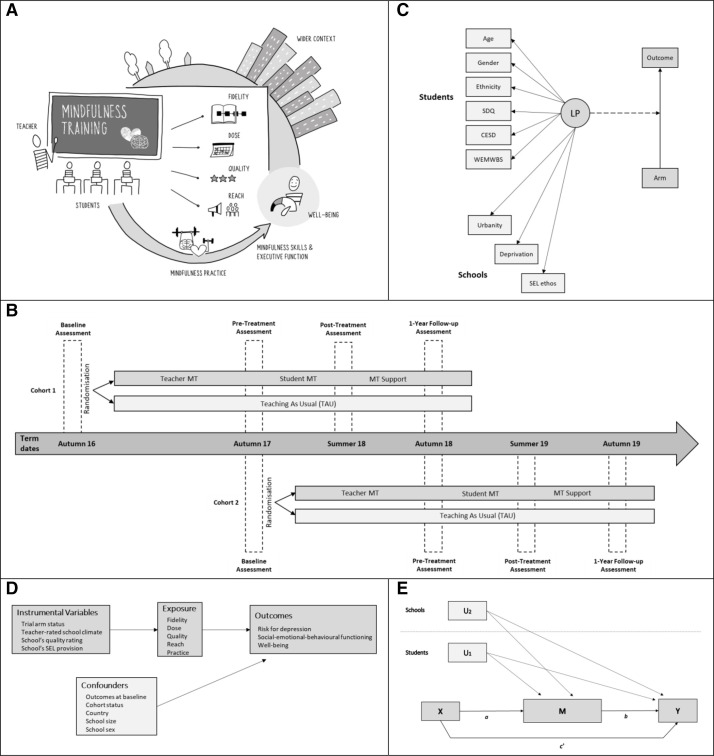
Methods: The My Resilience in Adolescence was a parallel-group, cluster randomised controlled trial (K=84 secondary schools; n=8376 students, age: 11-13) recruiting schools that provided standard social-emotional learning. Schools were randomised 1:1 to continue this provision (control/teaching as usual (TAU)), and/or to offer SBMT ('.b' (intervention)). Risk of depression, social-emotional-behavioural functioning and well-being were measured at baseline, preintervention, post intervention and 1 year follow-up. Hypothesised moderators, implementation factors and mediators were analysed using mixed effects linear regressions, instrumental variable methods and path analysis.
Findings: SBMT versus TAU resulted in worse scores on risk of depression and well-being in students at risk of mental health problems both at post intervention and 1-year follow-up, but differences were small and not clinically relevant. Higher dose and reach were associated with worse social-emotional-behavioural functioning at postintervention. No implementation factors were associated with outcomes at 1-year follow-up. Pregains-postgains in mindfulness skills and executive function predicted better outcomes at 1-year follow-up, but the SBMT was unsuccessful to teach these skills with clinical relevance.SBMT as delivered in this trial is not indicated as a universal intervention. Moreover, it may be contraindicated for students with existing/emerging mental health symptoms.
Clinical implications: Universal SBMT is not recommended in this format in early adolescence. Future research should explore social-emotional learning programmes adapted to the unique needs of young people.
Keywords: adolescence; implementation; mediation; mental health; moderation; preventive medicine; process evaluation; school-based mindfulness training.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: WK is the director of the Oxford Mindfulness Centre and receives royalties for several books on mindfulness. JMGW is former director of the Oxford Mindfulness Centre and receives royalties for several books on mindfulness.
Figures
References
-
- Greenberg MT. School‐based prevention: current status and future challenges. Effective Education 2010;2:27–52. 10.1080/19415531003616862 - DOI
Grants and funding
LinkOut - more resources
Full Text Sources